Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Smoking is a both a risk factor for developing rheumatoid arthritis (RA) and a predictor of severe, treatment-refractory disease in RA and other rheumatic conditions, yet, little is systematically done in rheumatology clinics to help patients quit smoking. We previously reported that only 10% of eligible RA visit notes documented tobacco counselling by rheumatologists; only one in 175 notes recommended quit line phone services. Quit line services are free in every state and recommended by US guidelines to improve quit rates four-fold, but are rarely leveraged in rheumatology clinics.
Methods: We designed a prospective study to examine the feasibility of a staff-led tobacco cessation intervention in three academic rheumatology clinics over six weeks in 2016, compared to 2012-2015. Medical assistants and nurses were educated on tobacco cessation and rehearsed evidence-based care in a one hour session. During clinic rooming, electronic health record (EHR) alerts prompted documentation of tobacco use, assessment of 30 day readiness to quit among users, and offers for electronic referral for quit line to phone the patient within one week. Process measures for assessing tobacco use and readiness to quit were compared (pre- post-) using standard EHR documentation fields. We compared quit line referral events to historic abstracted rates. Chi-square tests and logistic regression models were used to obtain odds ratios between the groups pre-intervention and during protocol implementation.
Results: Over the six week protocol pilot, 123 rheumatology visits with patients who smoke were compared to 4078 baseline visits with patients who smoke. Process measures showed that the protocol increased tobacco status documentation to 97% (OR 1.40, 95% CI 1.02-1.92) Table 1. Assessment of 30 day readiness to quit robustly increased from 3% before to 76% during the protocol intervention (OR 105, 65.7-167). Moreover, 32% (n=30) of those asked reported readiness to quit or cut back in the next 30 days. In total during the intervention, 12% (n=15 of 123 eligible visits) agreed to tobacco quit line electronic referral compared to 0.57% being offered referral (n=1 of 175) in our prior report (p<0.001).
Conclusion: The rheumatology staff protocol intervention for tobacco quit line electronic referral was feasible and tobacco cessation care improved by week six. A marked gain in assessing quit readiness, despite prior existence of this field in the EHR, shows that tools alone are ineffective and supports the need to study systematic implementation of such tools. A full six month pilot study is under way to assess protocol effectiveness including actual tobacco cessation rates. Given the importance of tobacco cessation for inflammatory disease activity and long term cardiovascular risk, methods should be studied to deliver tobacco cessation care or connect patients to proven quit resources. 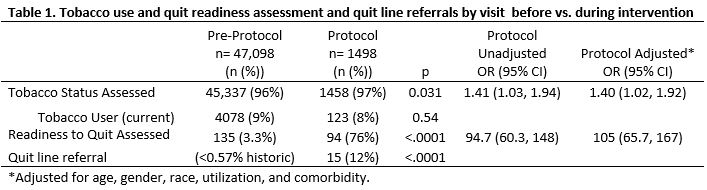
To cite this abstract in AMA style:
Bartels CM, Panyard D, Lauver D, Sampene E, Li Z, Adsit R, McBride P, Johnson H, Steffen Lewicki K, Ramly E. Feasibility of a Rheumatology Staff Protocol for Tobacco Cessation Counselling and Quit Line Electronic Referral [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/feasibility-of-a-rheumatology-staff-protocol-for-tobacco-cessation-counselling-and-quit-line-electronic-referral/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/feasibility-of-a-rheumatology-staff-protocol-for-tobacco-cessation-counselling-and-quit-line-electronic-referral/