Session Information
Date: Sunday, October 26, 2025
Title: (0731–0764) Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Giant Cell Arteritis (GCA) is a chronic, inflammatory condition, primary affecting the medium and larger arteries, usually in patients older than 50 years. It can lead to severe complications, being a cause of permanent loss of vision. Prompt diagnosis and treatment are essential to prevent severe outcomes. Traditional diagnostic pathways often involve lengthy delays due to the need for temporal artery biopsy, which can miss the diagnosis due to the segmental nature of the disease. Fast-Track Clinics (FTC) have emerged in response to this challenge as an innovative strategy to expedite diagnosis and treatment. However, to date, no comprehensive meta-analysis has been conducted to assess the effectiveness of FTC compared to conventional practice in GCA management. This study aims to fill that gap by providing the first pooled analysis of outcomes with FTC versus conventional care in GCA.
Methods: A systematic review and meta-analysis were conducted following PRISMA guidelines. Studies comparing FTC and CP in GCA were retrieved from MEDLINE, Cochrane, and Embase databases. Inclusion criteria required reporting at least one of the following outcomes: visual disturbances, permanent sight loss, biopsy rates, or median days to diagnosis. The QUADAS-2 tool was used for study quality and bias risk. Statistical analyses included pooled odds ratios (OR) with 95% confidence intervals (CI), heterogeneity assessment using the I² statistic, and a random-effects model to account for study variability. Funnel plots were used to assess publication bias.
Results: 348 patients were included across three studies (173 FTC group; 175 CP group – figure 1). Baseline characteristics are found in table 1. FTC implementation significantly reduced permanent sight loss (8.09% vs. 24.57%, OR 0.30; p < 0.001 – figure 2A), visual disturbances (20.23% vs. 32.57%, OR 0.53; p = 0.01 – figure 2B), and temporal artery biopsy (47.40% vs. 65.14%, OR 0.15; p = 0.05 – Figure 2C). Median days to diagnosis were slightly lower in the FTC group, though not statistically significant (Mean difference -1.11 days; p = 0.26 – figure 2D). Heterogeneity was low for permanent sight loss (I² = 0.00) and visual disturbances (I² = 0.00), but moderate to high for biopsy rates (I² = 0.82) and time to diagnosis (I² = 0.98). Publication bias was observed for biopsy rates and time to diagnosis.
Conclusion: This meta-analysis demonstrated that Fast-Track Clinics (FTC) improve clinical outcomes in Giant Cell Arteritis by significantly reducing the risk of permanent sight loss, decreasing the incidence of visual disturbances, and minimizing reliance on temporal artery biopsy. While reduction in diagnostic delay with FTC was not statistically significant, the overall findings support the integration of FTCs as an effective approach to expedite diagnosis and treatment in GCA.
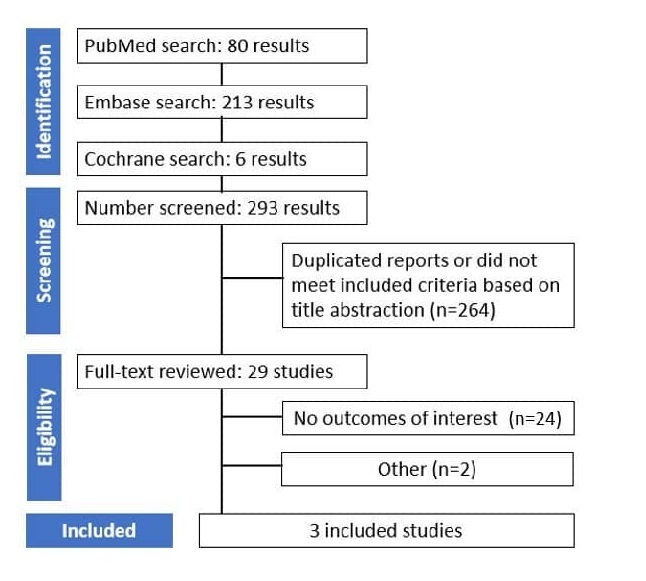 Figure 1 – PRIMA Box diagram of study screening and selection. PRISMA Box diagram of study screening and selection. The search strategy in Embase, MEDLINE and Cochrane yield 293 results, of which 29 were fully reviewed for inclusion and exclusion criteria. Three studies were included in the meta analysis
Figure 1 – PRIMA Box diagram of study screening and selection. PRISMA Box diagram of study screening and selection. The search strategy in Embase, MEDLINE and Cochrane yield 293 results, of which 29 were fully reviewed for inclusion and exclusion criteria. Three studies were included in the meta analysis
.jpg) Figure 2 – A: Permanent Sight Loss was inferior in Fast-Track Group (p-value = < 0.001); B; Visual disturbancies was inferior in Fast-Track Group (p-value = 0.01); C: Biopsy performed was inferior in Fast-Track Group (p-value = 0.05); D: Median Days performed was not statistically significant (p-value = 0.26)
Figure 2 – A: Permanent Sight Loss was inferior in Fast-Track Group (p-value = < 0.001); B; Visual disturbancies was inferior in Fast-Track Group (p-value = 0.01); C: Biopsy performed was inferior in Fast-Track Group (p-value = 0.05); D: Median Days performed was not statistically significant (p-value = 0.26)
.jpg) Table 1: Baseline characteristics Comparative Outcomes of Fast-Track Clinical Pathway vs Conventional Practice in Giant Cell Arteritis Management
Table 1: Baseline characteristics Comparative Outcomes of Fast-Track Clinical Pathway vs Conventional Practice in Giant Cell Arteritis Management
To cite this abstract in AMA style:
Beirão T, Rua C, Silva C, Patela M, Vieira R, Abelha-aleixo J, Pinto P, Costa F, Pinto A, Fonseca D, Meirinhos T, Souto A, Videira T. Fast-Track Clinics Improve Visual Outcomes in Giant Cell Arteritis: A Meta-Analysis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/fast-track-clinics-improve-visual-outcomes-in-giant-cell-arteritis-a-meta-analysis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/fast-track-clinics-improve-visual-outcomes-in-giant-cell-arteritis-a-meta-analysis/