Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Recent studies have reported that ultrasound features of urate crystal deposition are present in some asymptomatic individuals with hyperuricemia, suggesting that subclinical urate deposition occurs prior to presentation with symptomatic disease. Dual energy computed tomography (DECT) allows both specific detection and volume measurement of urate crystals. The aim of this study was to compare the frequency and volume of DECT urate deposits in people with asymptomatic hyperuricemia and symptomatic gout.
Methods: DECT scans of both feet were prospectively obtained from asymptomatic individuals with serum uric acid ≥9mg/dL recruited from community laboratories (n=25), and those with crystal proven gout without clinically apparent tophi (n=33). The gout group was separated into two groups: early gout (pre-defined as onset of symptoms in the preceding 3 years, n=14), and late gout (disease duration >3 years, n=19). Asymptomatic individuals with serum uric acid <6mg/dL (negative controls, n=10) and individuals with crystal proven tophaceous gout (positive controls, n=20) were studied to optimize the DECT settings. Two readers, blinded to all clinical features including gout status and serum uric acid, independently scored the scans for the presence and sites of urate deposition, and measured the urate volume in both feet using automated volume measurement software. For the purposes of analysis, DECT urate deposits were considered to be present if scored by both readers.
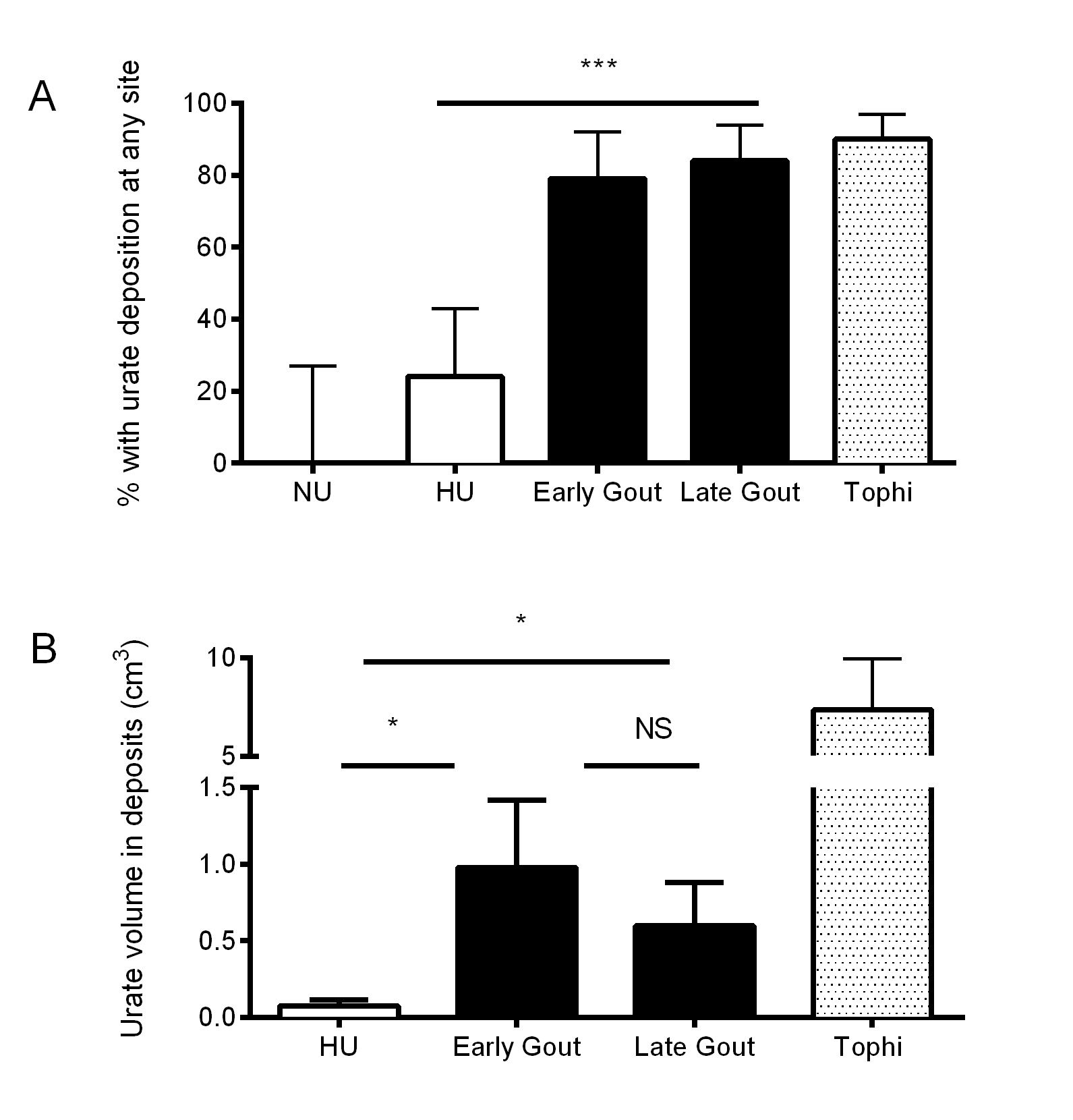
Results: DECT urate deposits were observed in 6/25 (24%) participants with asymptomatic hyperuricemia, 11/14 (79%) participants with early gout and 16/19 (84%) participants with late gout (p<0.001, Figure 1A). In those with urate deposits, the volume of urate deposition was significantly lower in those with asymptomatic hyperuricemia, compared with the early and the late gout groups (Kruskall-Wallis p=0.02, Figure 1B). Similar urate volumes were observed in the early and late gout groups (Figure 1B). DECT urate deposition was observed in both joints and tendons in the asymptomatic hyperuricemia group, but significantly less frequently than in both the early and late gout groups (p≤0.001 for both joint and tendon sites).
Conclusion: Although DECT can detect urate deposition in the feet of some asymptomatic individuals with hyperuricemia, these deposits are far more frequently observed in those with symptomatic gout. Urate deposit volumes are also greater in those with symptomatic disease. These data suggest that a threshold of urate crystal volume may be required before symptomatic gout occurs.
Figure: A. Frequency with urate deposition at any site, ***Chi-Square test p<0.001. B. Urate volume in those with deposits detected, *Dunn's multiple comparison test p<0.05. NU: asymptomatic normouricemia, HU: asymptomatic hyperuricemia.
Disclosure:
N. Dalbeth,
Ardea,
5,
AstraZeneca,
5,
Takeda,
5,
Metabolex,
5,
Menarini,
8,
Savient,
8,
Novartis Pharmaceutical Corporation,
8,
Fonterra,
2,
Novartis Pharmaceutical Corporation,
2,
Ardea,
2,
Fonterra,
9;
M. House,
None;
O. Aati,
None;
P. Tan,
None;
C. Franklin,
None;
A. Horne,
None;
G. Gamble,
None;
L. K. Stamp,
None;
A. Doyle,
None;
F. M. McQueen,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/extent-of-urate-deposition-in-asymptomatic-hyperuricemia-and-symptomatic-gout-a-dual-energy-computed-tomography-study/