Session Information
Date: Monday, November 14, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster III: Outcomes
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Patients with lupus nephritis (LN) are often treated with high doses of glucocorticoids and experience glucocorticoid-related toxicity. Quantifying this toxicity may be a useful tool both in clinical practice and in therapeutic trials. The glucocorticoid toxicity index (GTI) was developed by expert consensus to quantify accumulated toxicities from glucocorticoid treatments. To date, the GTI has not been evaluated in lupus nephritis, nor has it been shown to correlate with glucocorticoid exposure in this patient population.
Methods: We performed a single-center retrospective cohort study using the Beth Israel Deaconess Lupus Cohort, which was initiated in 2006. All patients enrolled in the cohort met the 1997 ACR diagnostic criteria for systemic lupus erythematosus. We included patients with biopsy-confirmed LN between 2006 and 2016 to have five years of available data post-biopsy for all patients. Cumulative glucocorticoid exposure was collected via medical record review from date of the diagnostic kidney biopsy through one- and five-years post-biopsy. Glucocorticoid dosing was converted to prednisone equivalents. The composite GTI was calculated using published methods using medical record review and adding the scores for all documented glucocorticoid-associated toxicities through one year and through five years post-biopsy. Positive points were given to worsening toxicities and negative points to improvement in toxicities. We performed linear regression to determine the association between cumulative glucocorticoid exposure and GTI scores through 1 year and 5 years following diagnosis.
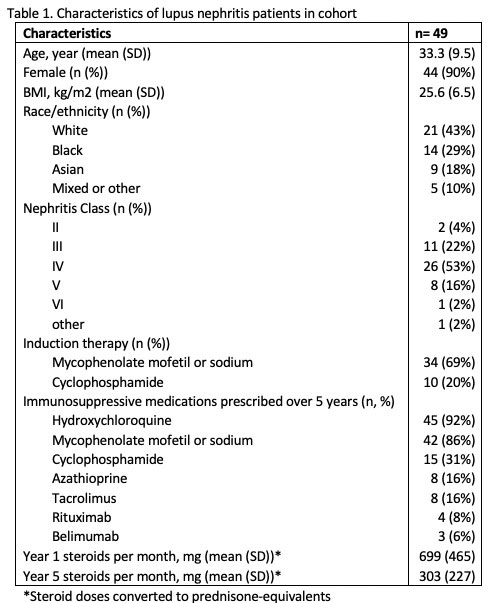
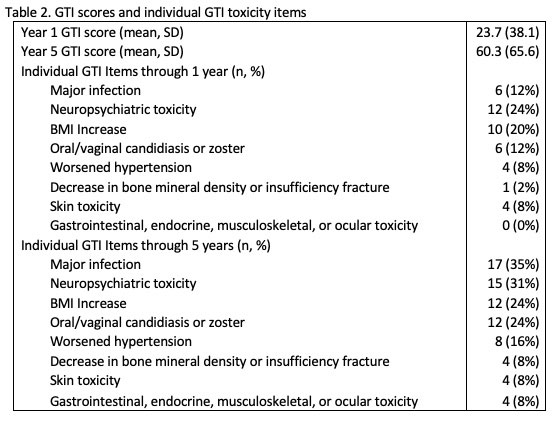
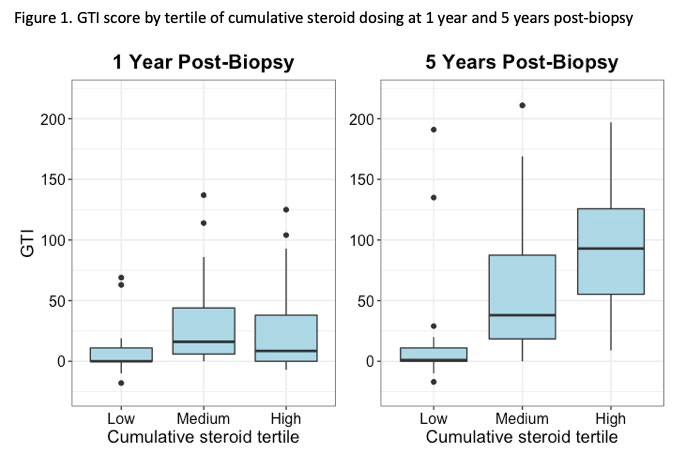
Results: We included 49 patients with biopsy-confirmed LN with a mean age of 33.3 (SD 9.5) years (Table 1). Patients had high cumulative glucocorticoid exposure, receiving an average of 699 mg prednisone-equivalents per month through year 1 and 303 mg prednisone-equivalents per month through year 5. The mean composite GTI was 23.7 (SD 38.1) through year 1 and 60.3 (SD 65.6) through year 5 (Table 2). At the end of the first year the most common glucocorticoid-related toxicities in the cohort were neuropsychiatric toxicities and increases in BMI. At the end of the fifth year, the most common toxicities were major infections, neuropsychiatric toxicities, and increases in BMI. Higher cumulative glucocorticoid exposure was associated with higher GTI through five years after diagnosis (p = 0.02); however, through year 1, glucocorticoid exposure was not associated with the GTI (p=0.63) (Figure 1).
Conclusion: Patients with LN are exposed to high cumulative doses of glucocorticoids and experience significant glucocorticoid-related morbidity. Our cohort experienced substantial neuropsychiatric and metabolic toxicities as well as serious infections. In this cohort study, the GTI was associated with cumulative steroid exposure during the 5 years after diagnosis, but was not associated with steroid exposure during the 1 year after diagnosis. In patients with LN, the GTI may be a more useful indicator of longer-term steroid toxicity than short-term toxicity and may serve as a useful outcome measure in future LN trials evaluating the steroid sparing effect of novel therapies.
To cite this abstract in AMA style:
Usiskin I, Kyttaris V. Estimating Corticosteroid-Related Morbidity in Lupus Nephritis: The Glucocorticoid Toxicity Index [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/estimating-corticosteroid-related-morbidity-in-lupus-nephritis-the-glucocorticoid-toxicity-index/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/estimating-corticosteroid-related-morbidity-in-lupus-nephritis-the-glucocorticoid-toxicity-index/