Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Smoking is a key risk factor for rheumatologic conditions such as rheumatoid arthritis and lupus that disproportionately impacts disadvantaged patients and predicts worse outcomes. Both smoking and rheumatic diseases increase risk for cardiovascular disease, yet rheumatology clinics address cessation in fewer than 10% of visits and offer referrals to free state-run tobacco quit lines (TQLs) in < 1% of visits. TQLs are proven to increase cessation 4-fold through free coaching and nicotine replacement.
Quit Connect supports rheumatology staff medical assistants or nurses with electronic health record (EHR) tools to Ask smokers about 30-day readiness to quit or cut back, Advise cessation support, and Connect ready patients via EHR orders to receive a TQL call (Figure 1). Quit Connect increased TQL referrals 26-fold in our prior study, and required < 90 seconds. We disseminated Quit Connect to the Grady Rheumatology Clinic, a public clinic in Atlanta, GA to test generalizability and increase TQL and smoking cessation class referrals.
Methods: We engaged medical assistants, nurses, clinic administrators, and rheumatologists to tailor Quit Connect implementation in a focus group. One-hour training offered cessation evidence and practice with talking points and EHR tools (Figure 2). Adults in the rheumatology clinic with current tobacco use were targeted. EHR tags captured process steps for when a patient was Asked about smoking/quit readiness, Advised regarding TQL and cessation class, or Connected via referral to TQL or cessation class. We compared performance before and after active implementation of the protocol, and we report 3 month midpoint data. Chi-square tests and unadjusted odds ratios compared findings months 1 to 3.
Results: At baseline, 83% of patients were Black, 40% were uninsured, and 52% received Medicare/Medicaid. During the 3 months of Quit Connect implementation, among 780 visits, 16% were smokers (Table 1). Among smokers, rates of triage staff asking readiness to quit increased from 13% in month 1 to 51% in month 3 (OR 8.6), compared to 0% before the project. Among smokers who were asked (n=30), 76% said that they were ready to quit or cut back in the next 30 days. Among those ready (n=23), 82% were offered referral to the TQL or class. Among those offered (n=19), 63% accepted the e-referral to the TQL and 68% accepted a referral to the class (p=0.99) compared to zero referred before Quit Connect implementation.
Conclusion: In a low resource rheumatology clinic with a majority of Black patients with limited insurance, many were ready to quit but had not been offered support. Within three months, Quit Connect dramatically increased referrals to a tobacco quit line and cessation class. This process is easily integrated into the EHR, engages staff, and leverages free, state-run resources for rheumatology patients. Monthly audit feedback will continue to encourage this brief intervention for rheumatology patients who smoke. Short and long-term outcomes will be evaluated including TQL reports of cessation attempts and patient outcomes. Future studies seek to scale out and disseminate Quit Connect in other populations and health systems.
 Figure 1. Quit Connect trains medical assistants and nurses to ASK smokers about readiness to quit, ADVISE cessation, and CONNECT patients to cessation resources such as a tobacco quit line or cessation class in under 90 seconds during clinic rooming.
Figure 1. Quit Connect trains medical assistants and nurses to ASK smokers about readiness to quit, ADVISE cessation, and CONNECT patients to cessation resources such as a tobacco quit line or cessation class in under 90 seconds during clinic rooming.
 Figure 2. Quit Connect implementation steps and timeline. Participants included study team, clinic manager, nurses, medical assistants and rheumatologists. Participants were engaged with a focus group and then trained with evidence-based information regarding effects of smoking on rheumatologic disease and how to connect patients to TQL or a cessation class using EHR referrals. Staff received monthly audit feedback regarding process of ASK, ADVISE, CONNECT to smoking cessation resources.
Figure 2. Quit Connect implementation steps and timeline. Participants included study team, clinic manager, nurses, medical assistants and rheumatologists. Participants were engaged with a focus group and then trained with evidence-based information regarding effects of smoking on rheumatologic disease and how to connect patients to TQL or a cessation class using EHR referrals. Staff received monthly audit feedback regarding process of ASK, ADVISE, CONNECT to smoking cessation resources.
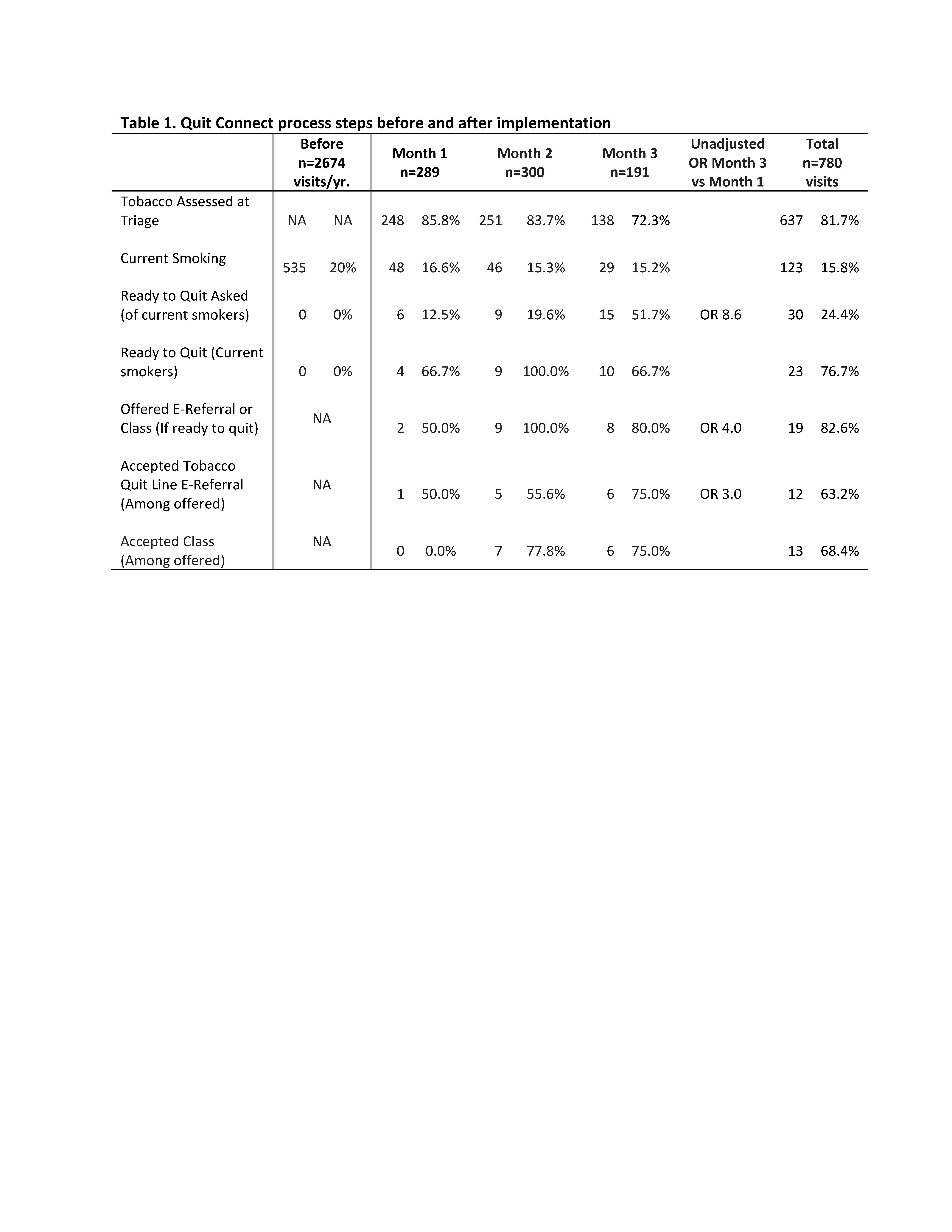 Table 1. Quit Connect process steps before and after implementation
Table 1. Quit Connect process steps before and after implementation
To cite this abstract in AMA style:
Brandt J, Lim S, Ramly E, Messina M, Bartels C. EHR-Supported Staff Protocol Improves Smoking Cessation in a Diverse Rheumatology Clinic: Results of Quit Connect Dissemination Project [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/ehr-supported-staff-protocol-improves-smoking-cessation-in-a-diverse-rheumatology-clinic-results-of-quit-connect-dissemination-project/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ehr-supported-staff-protocol-improves-smoking-cessation-in-a-diverse-rheumatology-clinic-results-of-quit-connect-dissemination-project/