Session Information
Session Type: ACR Concurrent Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Accelerated knee osteoarthritis (AKOA) is a unique endotype of knee osteoarthritis (KOA) that is characterized by a sudden onset of advance-stage disease and greater prodromal knee symptoms than those who develop a more gradual onset of KOA. Effusion-synovitis and infrapatellar fat pad (IFP) edema, may be potential early markers of AKOA because both are associated with pain and predict KOA incidence or progression. We aimed to determine whether greater effusion-synovitis and IFP edema on MRI differentiate incident AKOA from a gradual onset of KOA or no KOA.
Methods: We classified 3 sex-matched groups of participants in the Osteoarthritis Initiative who had a knee without radiographic KOA at baseline (Kellgren-Lawrence [KL]<2; n=125/group): 1) AKOA: ≥1 knee progressed to KL grade ≥3 within 48 months, 2) common KOA: ≥1 knee increased in radiographic scoring within 48 months without meeting AKOA criteria, 3) no KOA: both knees had the same KL grade at baseline and 48-months. Observation period included up to 2 years before and after an index visit, which was when the AKOA or common KOA criteria were met (no KOA index visit was matched to AKOA). Two musculoskeletal radiologists reported presence of IFP edema using the MOAKS grading system. Independent readers used a semi-automated method to segment intermediate-weighted fat-suppressed MRIs for effusion-synovitis volume and measurements were finalized by the senior reader. We used generalized linear mixed models with group and time as independent variables, as well as tested a group-by-time interaction.
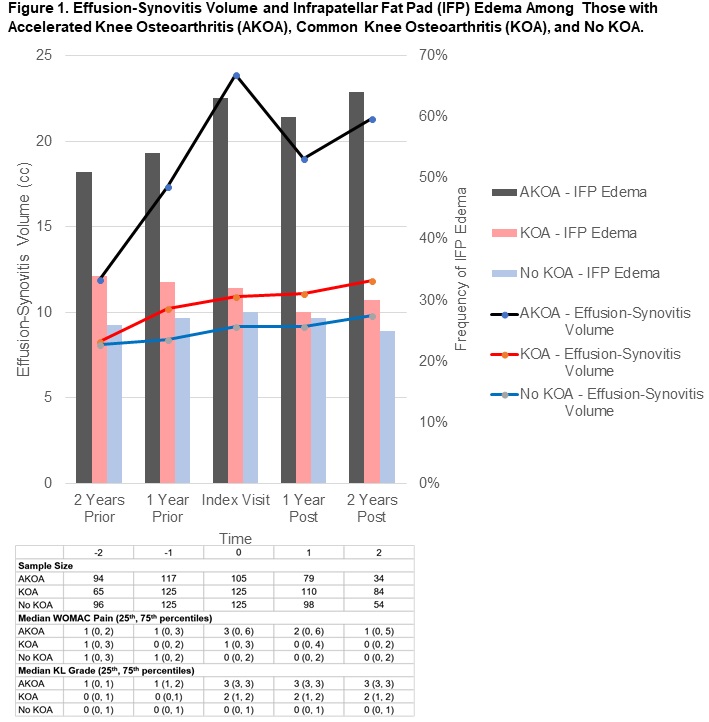
Results: Table 1 provides descriptive characteristics of each group. Starting at 2 years before disease onset and continuing to up to 2 years after onset, adults who developed AKOA had greater effusion-synovitis volume compared to adults with common or no KOA (p=0.015, p=0.003; Figure 1). Individuals who developed AKOA have at least two times the odds of having IFP edema compared to those with no KOA starting at 2 years prior to disease onset, and those with common KOA starting at 1 year prior to disease onset (Table 2, Figure 1).
Conclusion: As early as 2 years prior to disease onset AKOA is characterized by IFP edema and/or greater effusion-synovitis. Clinicians should be aware that people with greater effusion-synovitis and/or IFP edema in the absence of radiographic KOA may be at high risk for AKOA.
|
Table 1. Descriptive Characteristics of those with Accelerated Knee Osteoarthritis (AKOA), Common Knee Osteoarthritis (KOA), and No KOA at Osteoarthritis Initiative Baseline |
|||
|
(means, SD; except where noted) |
AKOA (n=125) |
Common KOA (n=125) |
No KOA (n=125) |
|
Females (n, %) |
79 (63%) |
79 (63%) |
79 (63%) |
|
Index knee KL Grade=0 (n, %) |
42 (34%) |
71 (57%) |
92 (74%) |
|
Patellofemoral Osteoarthritis (MR-based) (n, %) |
88 (75%) |
84 (69%) |
80 (66%) |
|
Frequent knee pain in past 12 months (n, %) |
44 (35%) |
49 (39%) |
30 (24%) |
|
Age (years) |
62.5 (8.5) |
58.4 (8.4) |
57.3 (8.2) |
|
Body mass index (kg/m2) |
29.7 (4.6) |
28.1 (4.4) |
26.9 (4.4) |
|
Global impact rating (0 to 10; higher score=greater impact) |
1.7 (1.9) |
1.1 (1.5) |
0.8 (1.1) |
|
How many days limited activities in past 30 days (0 to 30)? |
3.2 (7.3) |
1.7 (4.8) |
1.4 (4.3) |
|
WOMAC pain (0 to 20; higher score=more pain) |
2.3 (3.1) |
1.8 (2.3) |
1.6 (2.4) |
|
Notes: SD = standard deviation, KL = Kellgren-Lawrence, MR = magnetic resonance |
|||
|
Table 2. Adults with Accelerated Knee Osteoarthritis (AKOA) Have Twice the Odds of Having Infrapatellar Fat Pad Edema Than those with Common Knee Osteoarthritis (KOA), and No KOA (n = 125/group) |
||||
|
Outcome |
Visit |
|
|
|
|
Infrapatellar Fat Pad Edema (OR [95% CI]) |
AKOA vs No KOA (REF) |
Common KOA vs No KOA (REF) |
AKOA vs Common KOA (REF) |
|
|
-2 |
2.07 (1.14, 3.78) |
1.67 (0.90, 3.08) |
1.24 (0.69, 2.25) |
|
|
-1 |
3.06 (1.71, 5.48) |
1.46 (0.82, 2.60) |
2.10 (1.19, 3.69) |
|
|
Index |
3.68 (2.07, 6.57) |
1.18 (0.68, 2.06) |
3.12 (1.79, 5.44) |
|
|
1 |
3.66 (2.04, 6.57) |
1.05 (0.60, 1.85) |
3.48 (1.97, 6.16) |
|
|
2 |
3.95 (2.09, 7.46) |
1.06 (0.59, 1.92) |
3.72 (2.01, 6.87) |
|
|
Notes: OR=Odds Ratio. CI=Confidence Interval. REF= reference group. Group-by-time interaction: p<0.001). Infrapatellar fat pad edema was assessed on intermediate-weighted fat-suppressed magnetic resonance images. |
||||
To cite this abstract in AMA style:
Davis J, Ward RJ, MacKay J, Lu B, Price LL, McAlindon TE, Eaton CB, Barbe M, Lo GH, Harkey M, Driban JB. Effusion-Synovitis and Infrapatellar Fat Pad Edema Differentiate Accelerated Knee Osteoarthritis: Data from the Osteoarthritis Initiative [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/effusion-synovitis-and-infrapatellar-fat-pad-edema-differentiate-accelerated-knee-osteoarthritis-data-from-the-osteoarthritis-initiative/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/effusion-synovitis-and-infrapatellar-fat-pad-edema-differentiate-accelerated-knee-osteoarthritis-data-from-the-osteoarthritis-initiative/