Session Information
Date: Tuesday, November 14, 2023
Title: Abstracts: Spondyloarthritis Including Psoriatic Arthritis – Treatment III: AxSpA
Session Type: Abstract Session
Session Time: 4:00PM-5:30PM
Background/Purpose: While subcutaneous secukinumab (SEC) is approved for the treatment of axial spondyloarthritis (axSpA), some patients may benefit more from intravenous (IV) administration. This study investigated the long-term efficacy, safety, and tolerability of IV SEC in patients with active axSpA.
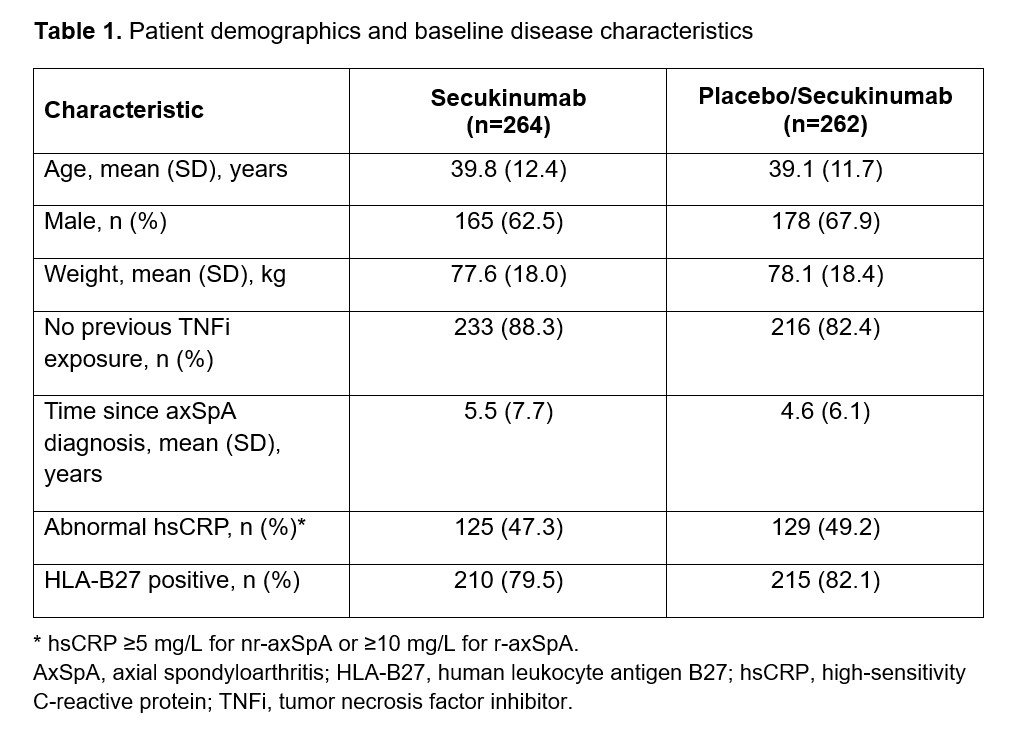
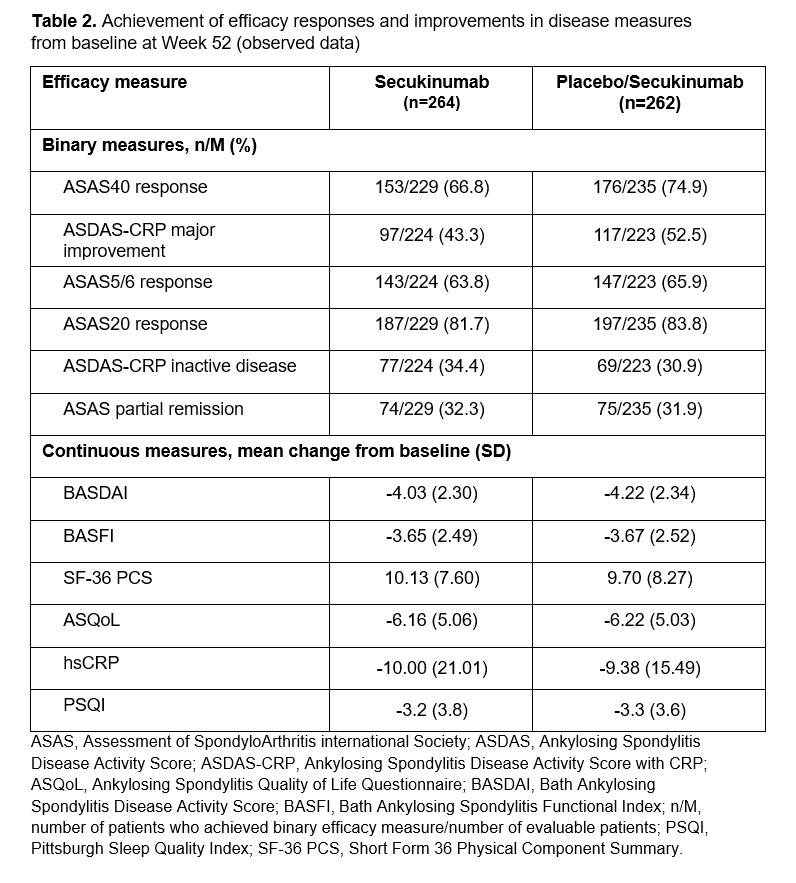
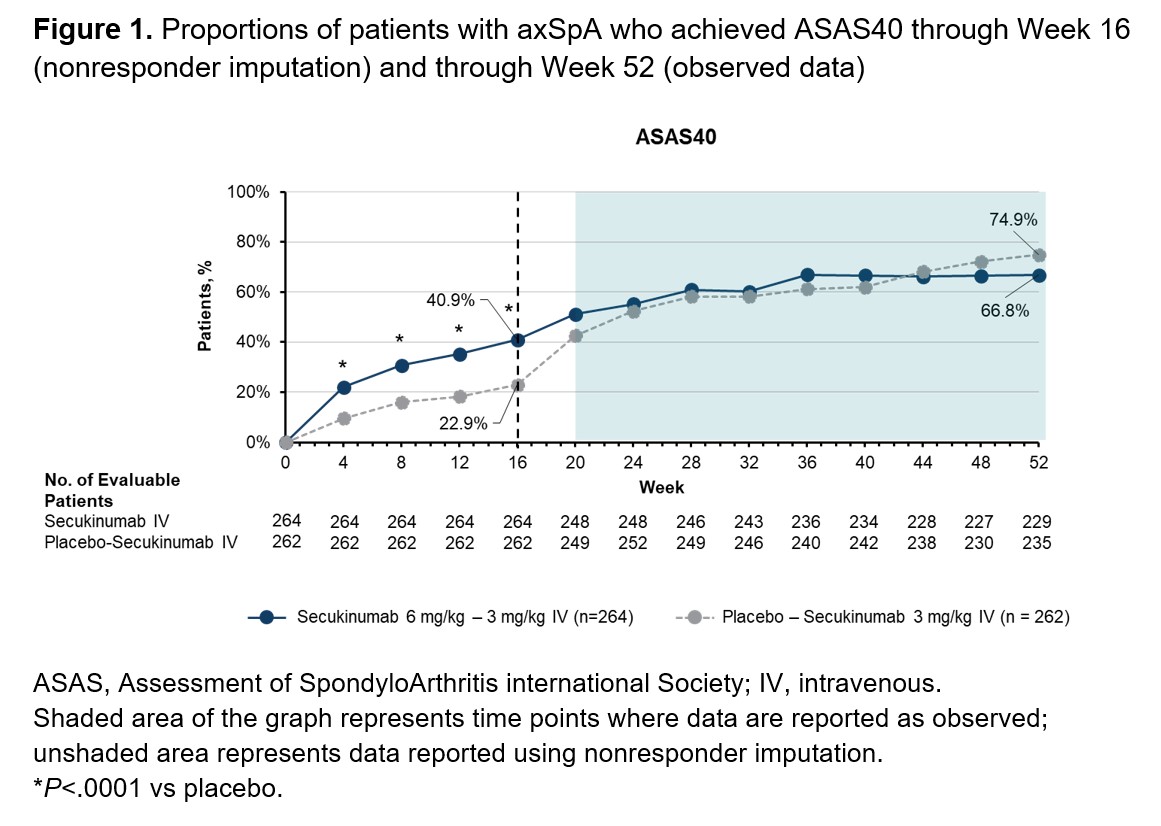
Methods: INVIGORATE-1 (NCT04156620) is a randomized, double blind, parallel group, phase 3 trial of patients with active axSpA (either radiographic [r]-axSpA or nonradiographic [nr]-axSpA). All patients had inflammatory back pain (ASAS criteria) for ≥6 months with onset before 45 years of age. Patients with r-axSpA fulfilled the modified New York criteria, and patients with nr-axSpA met ASAS criteria and had objective signs of inflammation at screening (positive MRI and/or elevated high-sensitivity C-reactive protein (≥5 mg/L for nr-axSpA; ≥10 mg/L for r-axSpA). Patients were randomized 1:1 to receive IV SEC (6 mg/kg at baseline followed by 3 mg/kg every 4 weeks) or placebo (PBO) for 16 weeks. After Week 16, patients randomized to PBO were switched to IV SEC (3 mg/kg every 4 weeks), while patients randomized to SEC continued receiving IV SEC through Week 52. The primary endpoint was ASAS40 response at Week 16. Efficacy was assessed through Week 52 by the proportion of patients achieving ASAS40 response, ASDAS-CRP major improvement, and ASAS5/6 response, and by change from baseline in BASDAI, BASFI, and SF-36 PCS. Safety was evaluated through Week 60. Efficacy data through Week 16 are reported using nonresponder imputation; efficacy data from Week 20 through Week 52 are reported as observed.
Results: Demographics and baseline characteristics were balanced across treatment groups (Table 1). Among patients randomized to IV SEC (n=264) or PBO/IV SEC (n=262), 86.0% and 88.9% completed the entire study period, respectively. A total of 413 patients had r-axSpA and 113 patients had nr-axSpA. SEC treatment resulted in rapid and sustained improvement in ASAS40 response rates in patients randomized to SEC (Figure 1). By Week 24, patients who switched from PBO to SEC at Week 16 achieved comparable ASAS40 response rates to those of patients originally randomized to SEC. ASAS40 responses were maintained through Week 52 for both groups (SEC, 66.8%; PBO/IV SEC, 74.9% [observed data]). SEC treatment also resulted in rapid improvements in all other efficacy measures that were maintained through Week 52 (Table 2). Through Week 16, the incidences of adverse events (AEs; 38.6% vs 39.1%), serious AEs (2.7% vs 1.1%), and AEs leading to treatment discontinuation (1.9% vs 0.4%) were similar for patients receiving SEC or PBO, respectively. Among patients receiving any IV SEC through the entire study period, 63.2%, 6.0%, and 3.5% reported any AE, serious AEs, and AEs leading to treatment discontinuation, respectively. One death occurred during SEC treatment due to a suspected myocardial infarction and was deemed not related to treatment.
Conclusion: IV SEC was safe and effective for treatment of adults with active axSpA over 52 weeks. The safety profile of IV SEC for patients with axSpA was consistent with that of previous reports for subcutaneous SEC, and no new safety signals were observed.
To cite this abstract in AMA style:
Deodhar A, Supronik J, Kivitz A, Valenzuela G, Kapur K, Rohrer S, Dokoupilova E, Richards H, Pavelka K. Efficacy and Safety of Intravenous Secukinumab for the Treatment of Active Axial Spondyloarthritis: Results from a Randomized, Double-Blind, Phase 3 Study [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/efficacy-and-safety-of-intravenous-secukinumab-for-the-treatment-of-active-axial-spondyloarthritis-results-from-a-randomized-double-blind-phase-3-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/efficacy-and-safety-of-intravenous-secukinumab-for-the-treatment-of-active-axial-spondyloarthritis-results-from-a-randomized-double-blind-phase-3-study/