Session Information
Date: Sunday, November 13, 2022
Title: Pediatric Rheumatology – Clinical Poster II: Connective Tissue Disease
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Childhood onset SLE is an autoantibody mediated, multisystem disease which can include cardiac manifestations. Because cardiac involvement can develop insidiously, an earlier review from our center suggested that routine echocardiogram (ECHO) screening could allow earlier recognition. We therefore implemented a quality improvement initiative with routine ECHO screening following diagnosis and then two yearly, or as indicated if abnormalities were identified. The aim of this study is to determine the frequency and type of abnormal ECHO findings identified when testing performed as routine screening or for clinical indication in children with SLE followed at BC Children’s Hospital and to determine the association with disease activity.
Methods: All children (< 18 years) diagnosed with SLE from 2005 to 2015 were identified from our records (cutaneous or drug induced lupus were excluded). By chart review we collected all ECHO and EKG results and clinical data both at diagnosis and at time of ECHO testing including SLEDAI score and ESR as disease activity measures.
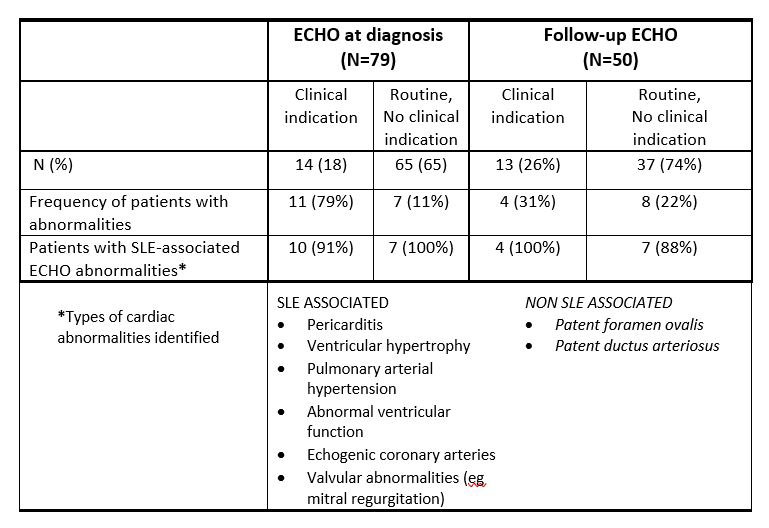
Results: 81 children with SLE were identified. At diagnosis, mean age was 13.4y; mean SLEDAI score was 13.2 (range 1-45), and mean ESR 56.3 (range 10-136); 98% (79/81) had at least one ECHO. The median interval from diagnosis to first ECHO was 1.5m (range 0-32); the mean associated SLEDAI score was 9 (range 0-32) and ESR 42.3 (range 3-136). Initial ECHO was requested routinely in 82% (65/79) and for clinical indication in 18% (14/79). Of the 23% (18/79) with abnormalities, mean SLEDAI was 14.3 (range 1-32) and ESR 68 (range 7-136). Of the 77% (61/79) with no abnormalities, mean SLEDAI was 7.3 (range 0-32) and ESR 34.6 (range 3-122). ECHO abnormalities were found in 11% (7/65) of patients routinely tested with no clinical indications and in 79% (11/14) with clinical indication. Abnormalities identified are shown in the table and include pericardial effusion, thickened left ventricular wall likely SLE related and PFO and PDA, likely congenital.
62% (50/81) had at least two echocardiograms with median time interval from diagnosis to second ECHO 24.7m (range 0.3-71.7m). The mean SLEDAI at second ECHO was 4.9 (range 0-32), ESR was 20.4 (range 4-132). The mean SLEDAI score of the 12 patients with an abnormal second ECHO was 7 with ESR 26.2. 6/12 (50%) did not have abnormalities on initial ECHO; one of these was performed for clinical indication and showed a new abnormality. 2/12 had previous abnormality and were noted to have progressive worsening.
Conclusion: Among children diagnosed with SLE, 23% were identified by ECHO with cardiac abnormalities; of these 61% had a cardiac clinical indication for testing and 39% were tested as a ‘routine’ practice. The frequency of ECHO abnormalities suggest testing soon after diagnosis may identify SLE and non-SLE abnormalities for comparison against future tests done routinely, or for clinical indication and to determine evolution of changes. SLEDAI score and ESR were not predictive of positive echocardiographic findings, though did tend to be higher than the entire group. This review may inform the utility and optimal practice of echocardiographic screening in pediatric SLE.
To cite this abstract in AMA style:
Marsden A, Tiller G, Rivera A, Rai M, Tucker L, Guzman J, Morishita K, Houghton K, Moodley S, Cabral D. Echocardiographic Screening in Childhood Onset Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/echocardiographic-screening-in-childhood-onset-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/echocardiographic-screening-in-childhood-onset-systemic-lupus-erythematosus/