Session Information
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: To examine the diagnostic accuracy of dual-energy computed tomography (DECT) vs. ultrasound or their combination for the diagnosis of gout.
Methods: Using data from an outpatient rheumatology clinic, we examined the sensitivity, specificity, positive and negative predictive value (PPV, NPV) and area under the receiver operating characteristic (ROC) curve (AUC) of either modality or their combination for gout diagnosis. We used two standards: (1) demonstration of monosodium urate (MSU) crystals in synovial fluid (gold); and (2) 2015 American College of Rheumatology and European League Against Rheumatism (ACR-EULAR) classification criteria for gout, modified to exclude points based on DECT and ultrasound findings (silver), since these were test standards.
Results: Of the 147 patients who provided data, 48 had synovial fluid analysis performed (38 had MSU crystals and 10 were MSU-crystal negative). The mean age of 64.7 years (standard deviation, 14.3) and a mean symptom duration of 9.2 years. 113 (77%) met the silver standard, i.e. modified ACR-EULAR classification criteria for gout, and 34 (23%) did not.
Compared to the gold standard of synovial fluid MSU crystal positivity, the accuracy statistics for feet DECT, knee DECT, feet ultrasound double contour (DC) sign, combined feet DECT and feet ultrasound diagnosis (DC sign or tophus), and combined knee and feet DECT and ultrasound were: (1) sensitivity, 87%, 91%, 76%, 95%, 97%; (2) specificity, 100%, 87%, 60%, 60%, 50%; (3) PPV, 100%, 97%, 88%, 90%, 88%; (4) NPV, 67%, 75%, 40%, 70%, 83%; (5) AUC, 0.93, 0.89, 0.68, 0.77, and 0.74 (Table 1). These findings were replicated compared to the modified ACR-EULAR gout classification criteria, but with lower numbers (Table 2). Feet DECT, followed by knee DECT had the highest accuracy for the diagnosis of gout (Figure 2); ultrasound DC sign or the combination of DECT and ultrasound or across joints had lower accuracy.
Conclusion: In a single-center rheumatology clinic study, feet or knee DECT had the best overall accuracy statistics for the diagnosis of gout. DECT/ultrasound combination or multiple joint imaging may offer no additional increase in overall diagnostic accuracy.
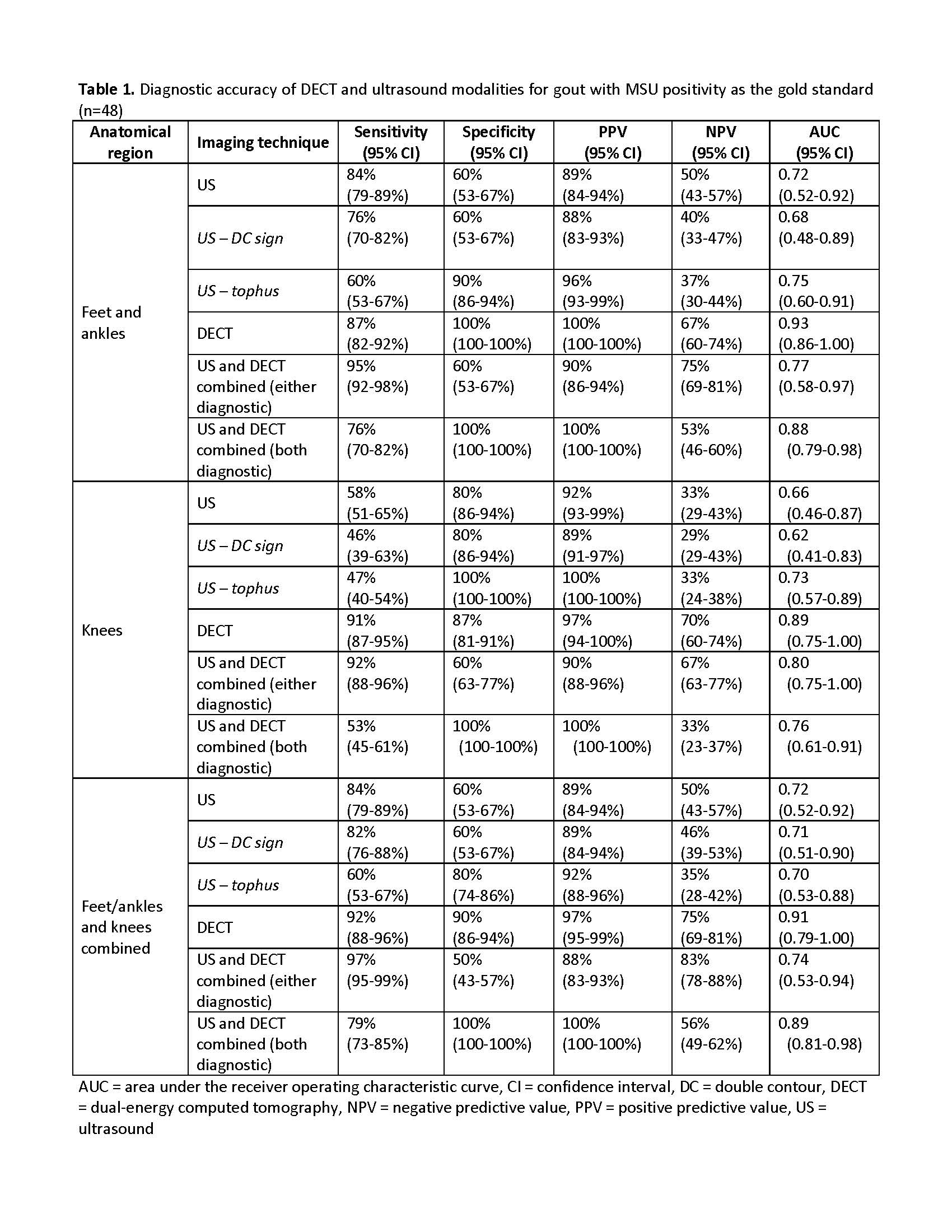 Table 1. Diagnostic accuracy of DECT and ultrasound modalities for gout with MSU positivity as the gold standard (n=48)
Table 1. Diagnostic accuracy of DECT and ultrasound modalities for gout with MSU positivity as the gold standard (n=48)
 Table 2. Diagnostic accuracy of DECT and ultrasound modalities for gout with modified ACR/EULAR gout classification criteria as the silver standard (N=147)
Table 2. Diagnostic accuracy of DECT and ultrasound modalities for gout with modified ACR/EULAR gout classification criteria as the silver standard (N=147)
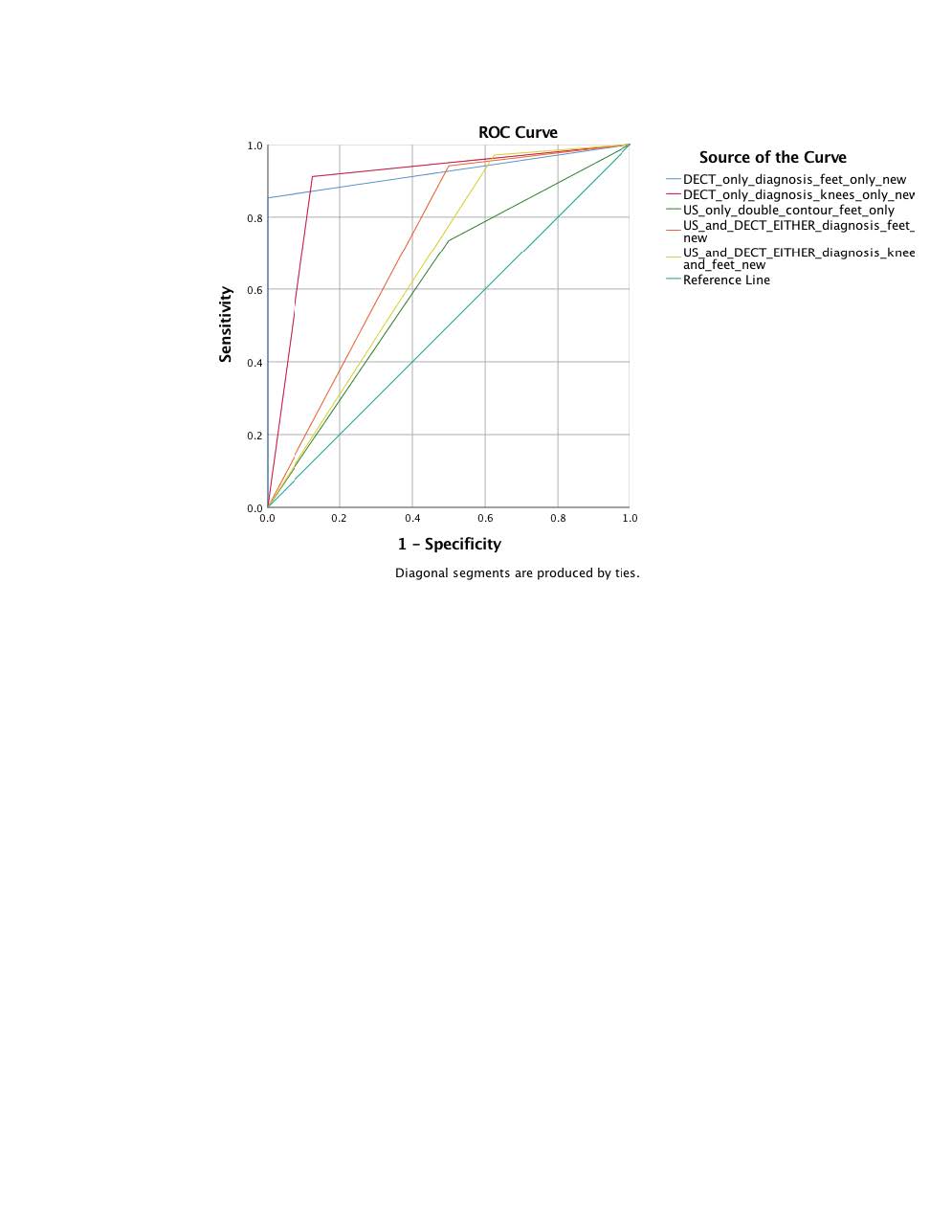 Figure 1. Area under the curve for the DECT and ultrasound modalities, alone or combined for feet/ankles, knees and both areas combined against the gold standard of synovial fluid monosodium urate (MSU) crystals Figure legend: The X-axis represents 1-specificity and Y-axis represents sensitivity. The null hypothesis is the diagonal line with an area of 0.50; the greater the area, the higher the overall accuracy of each modality. The area was highest for feet DECT (0.93) and lowest for feet ultrasound double contour (DC) sign (0.68).
Figure 1. Area under the curve for the DECT and ultrasound modalities, alone or combined for feet/ankles, knees and both areas combined against the gold standard of synovial fluid monosodium urate (MSU) crystals Figure legend: The X-axis represents 1-specificity and Y-axis represents sensitivity. The null hypothesis is the diagonal line with an area of 0.50; the greater the area, the higher the overall accuracy of each modality. The area was highest for feet DECT (0.93) and lowest for feet ultrasound double contour (DC) sign (0.68).
To cite this abstract in AMA style:
Singh J, Becce F, Budzik J, Pascart T. Dual-energy CT versus Ultrasound, Alone or in Combination, for the Diagnosis of Gout: A Diagnostic Performance Study [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/dual-energy-ct-versus-ultrasound-alone-or-in-combination-for-the-diagnosis-of-gout-a-diagnostic-performance-study/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/dual-energy-ct-versus-ultrasound-alone-or-in-combination-for-the-diagnosis-of-gout-a-diagnostic-performance-study/