Session Information
Date: Monday, October 22, 2018
Title: Metabolic and Crystal Arthropathies – Basic and Clinical Science Poster I
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Gout is associated with joint damage, and increased cardiovascular morbidity, so to diagnose and treat gout early is important. However, joint aspiration and microscopy not always yield the diagnosis. The latest diagnostic technique to visualize monosodium uric acid (MSU) depositions is Dual Energy CT scan (DECT).1
We purpose to assess the sensitivity and specificity of DECT for diagnosing gout in patients with unclassified arthritis.
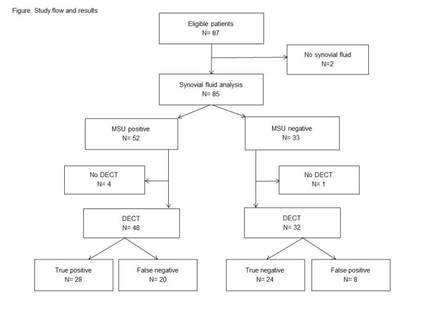
Methods: We included 87 consecutive patients with acute mono or oligo arthritis without prior gout diagnosis who presented to the outpatient clinic of the Department of Rheumatology of Meander Medical Centre, Amersfoort, the Netherlands, ClinicalTrials.gov number NCT03038386. Seven patients dropped out, see Figure. Patients underwent aspiration of the arthritic joint for the detection of MSU crystals (see Table) and a DECT scan of hands and wrists, knees, ankles and feet. The synovial fluid result for MSU crystals was the gold standard for gout.
Results: For demographic and clinical characteristics of the patients see Table, and for study data and outcomes see Figure. The sensitivity and specificity of DECT for gout deposition in the index joint were 0.58 (95% CI 0.43-0.72) and 0.75 (95% CI 0.57-0.89), respectively, with an area under the ROC curve of 0.67 (95% CI 0.55-0.79), p<0.05. When classifying DECT as positive if deposition was observed at the index joint and/or in other locations, sensitivity was higher: 0.77 (95% CI 0.63-0.88), but specificity lower: 0.69 (95% CI 0.48-0.86).
Conclusion: These preliminary data show the diagnostic value of DECT in patients with acute unclassified mono or oligo arthritis. Probably, DECT sensitivity is underestimated by false negative MSU results due to a sampling error, because of incorrect aspiration, or extra-articular locations of the gout, e.g. around tendons.
Table. The demographic and clinical characteristics of the patients (n=80) included in the study
|
Patients MSU positive (n=48) |
Patients MSU negative (n=32) |
|
|
Age in years, mean (SD), |
59.0 (15.6) |
63.1 (13.0) |
|
Sex, N (%) |
||
|
Male
|
41 (85.4)
|
25 (78.1)
|
|
Female
|
7 (14.6)
|
7 (21.9)
|
|
Arthritic joint aspirated (N, %) |
||
|
MTP1 |
29 (60.4)
|
6 (18.8)
|
|
Other joints |
19 (39.6)
|
26 (81.2)
|
|
Period between 1th arthritis attack and baseline visit in months, median (IQR)* |
12 (56) |
6 (35.8) |
|
Serum uric acid (µmol/L) mean (SD) |
465.72 (120.65)
|
403.50 (109.71)
|
* according to patient
To cite this abstract in AMA style:
Gamala M, Jacobs JWG, Linn-Rasker S, Nix M, Heggelman B, Pasker P, van Laar J, Klaasen R. Dual-Energy CT for the Diagnosis of Gout: A Prospective Study in Patients with No Prior History of Gout [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/dual-energy-ct-for-the-diagnosis-of-gout-a-prospective-study-in-patients-with-no-prior-history-of-gout/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/dual-energy-ct-for-the-diagnosis-of-gout-a-prospective-study-in-patients-with-no-prior-history-of-gout/