Session Information
Date: Tuesday, November 7, 2017
Title: Rheumatoid Arthritis – Clinical Aspects Poster III: Comorbidities
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Galectin-3 is a beta-galactoside-binding lectin and is a marker of cardiovascular disease (CVD) in the general population. However, galectin-3 level is also elevated in RA sera and synovia. Thus, its utility as a biomarker of subclinical cardiac pathology in RA patients is not established. We investigated the association between galectin-3 levels and measures of cardiac structure and function in a cohort of patients with RA and no known clinical CVD.
Methods: RA patients (n=114) without clinical CVD participated in a prospective cohort study and underwent 3D echocardiography and cardiac (18F-fluorodeoxyglucose [FDG]) positron emission-computed tomography. FDG uptake in aorta and in myocardium, measured as standardized uptake values (SUV), was available in 88 and 97 participants respectively. Linear regression models were used to explore the associations of galectin-3 levels with RA patient characteristics, left ventricular mass index (LVMI), and SUVs.
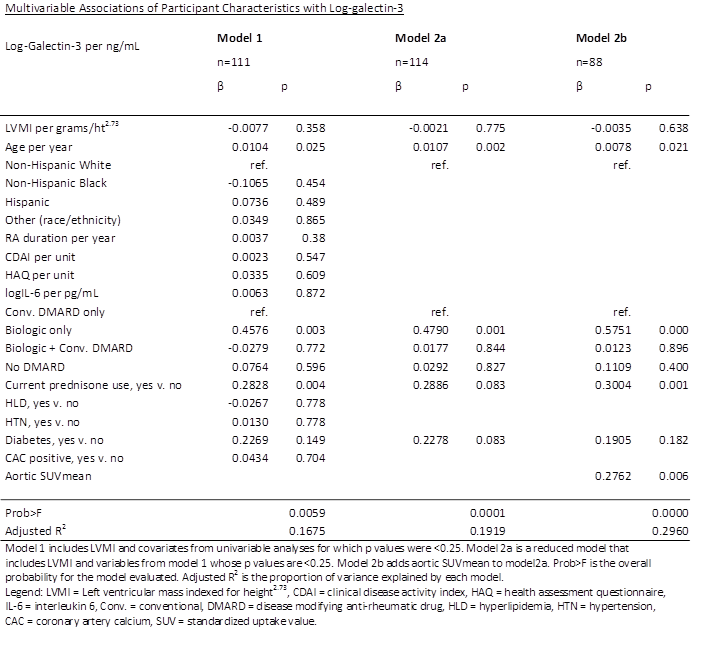
Results: A total of 114 RA patients [mean age 56 years; 80% female; 36% White, 15% non-Hispanic Black, 44% Hispanic; Median RA duration 6.9 years; 77% RF or anti-CCP positive; Median CDAI 15.8; 51% treated with only conventional DMARD, 29% treated with conventional DMARD and biologic, 10% treated with biologic only, 10% treated with no DMARD; 38% on prednisone] were analyzed. Median galectin-3 level was 8.26 ng/mL. In univariate analyses, galectin-3 levels were significantly and positively correlated with age, Hispanic ethnicity, RA duration, IL-6 level, treatment with biologic only, prednisone use, diabetes, and aortic SUVmean, but not with LVMI or myocardial SUV. In an adjusted multivariable model (Model 2a), age (β=0.0107, p=0.002) and treatment with biologic only (β= 0.4790, p=0.001) remained significantly associated with galectin-3 level. In an additional model adding aortic SUVmean (n=88) (Model 2b), prednisone use (β=0.3073, p=0.000) and aortic SUVmean (β=0.2803, p=0.0004) were significantly associated with galectin-3 level.
Conclusion: Age, treatment with biologic only, prednisone use, and aortic inflammation were associated with higher galectin-3 levels in RA patients without clinical CVD disease, while LVMI and myocardial inflammation were not. Galectin-3 was not an independent marker of higher LV mass (a precursor of heart failure) in this RA cohort, but additional measures of LV structure and function will be examined.
To cite this abstract in AMA style:
Nussdorf A, Amigues I, Bathon J. Does Galectin-3 Have Utility As a Biomarker of Subclinical Cardiovascular Disease in RA Patients Independently of RA Disease Activity? [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/does-galectin-3-have-utility-as-a-biomarker-of-subclinical-cardiovascular-disease-in-ra-patients-independently-of-ra-disease-activity/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/does-galectin-3-have-utility-as-a-biomarker-of-subclinical-cardiovascular-disease-in-ra-patients-independently-of-ra-disease-activity/