Session Information
Date: Monday, November 14, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster III: Outcomes
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose:
Background: Early complete remission (within 12 months from diagnosis) is considered an important protective factor against development of advanced chronic kidney disease (CKD) in lupus nephritis (LN). However, a certain proportion of such patients still develop advanced CKD and, eventually, end-stage renal disease (ESRD).
Objective: To describe the factors associated with the development of advanced CKD (stage IV or worse) in patients with LN who achieved early complete remission.
Methods: Patients with LN based on biopsy or abnormal proteinuria ( >0.5g/day) and/or hematuria or pyuria or casts for two consecutive visits in the absence of any other plausible explanation were retrieved from the Toronto Lupus Clinic longitudinal database. Individuals with advanced CKD at baseline (eGFR≦29ml/min/1.73m2) were excluded. All patients achieved complete remission (proteinuria< 0.5g/24h, inactive urinary sediment and serum creatinine £120% of baseline) within 12 months. Flare was defined as any abnormal proteinuria ( >0.5g/day) or increase in serum creatinine (SCR) from normal to abnormal or >120% of baseline after remission plus treatment escalation (glucocorticoids and/or immunosuppressives).
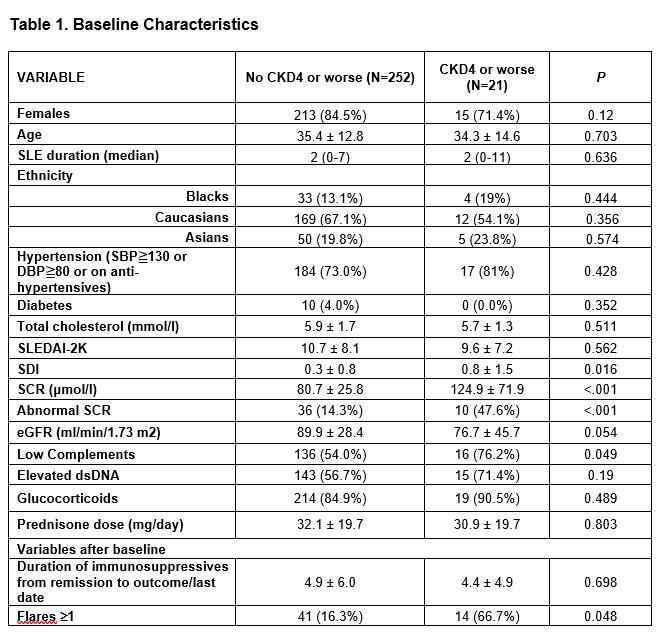
Results: Of 273 eligible patients achieving remission within the first year, 21 (7.7%) developed advanced CKD after a median of 5.8 years from the time of remission (range 0.7-31.7 years). The baseline characteristics are shown in Table 1.
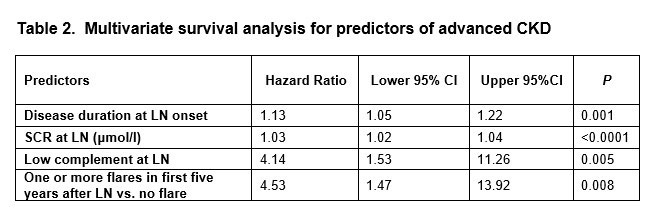
Multivariate survival analysis for predictors of advanced CKD is shown in Table 2.
We further divided the 21 patients who developed advanced CKD according to the median time (5.9 years). Patients who developed CKD early were older (44.2±16.7 vs. 26.8±6.7 years, p=0.004), had lower eGFR (52±44 vs. 96±39ml/min/1.73m2, p=0.022), lower SLEDAI-2K (6.5±5.2 vs. 12.8±7.4, p=0.03) and were more often treated with antihypertensives (63.6% vs. 18.2%, p=0.03) compared to the late progressors. The major factors leading to early advanced CKD were poor compliance or insufficient therapy due to concomitant infections in 7 and moderate-to-severe interstitial fibrosis and tubular atrophy (IFTA) in 4 patients. In late progressors, compliance was poor in 2 patients, moderate-to-severe IFTA was present in 3, poorly controlled hypertension in 2, thrombotic microangiopathy in one, refractory disease in one while one patient progressed very slowly over 32 years.
Conclusion: Patients with impaired kidney function and low complement C3 at baseline, as well as histopathologic features of chronic irreversible damage (interstitial fibrosis/tubular atrophy), are at risk for CKD despite early remission and should be followed closely. The importance of maintenance therapy should be communicated to the patients to prevent non-compliance and subsequent flares.
To cite this abstract in AMA style:
TSELIOS K, Gladman D, Su J, Urowitz M. Does Early Complete Remission Preclude Adverse Outcomes in Lupus Nephritis? [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/does-early-complete-remission-preclude-adverse-outcomes-in-lupus-nephritis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/does-early-complete-remission-preclude-adverse-outcomes-in-lupus-nephritis/