Session Information
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Although women are twice as likely as men to develop myositis, Black women are affected disproportionately. Additionally, minorities with juvenile dermatomyositis are significantly more likely to have low family income and significantly worse scores on physical function, disease activity and quality of life. This pilot study investigates the relationship between race/ethnicity, sex, living in a disadvantaged neighborhood, and the frequency of being prescribed a DMARD (biologic or conventional) or a steroid in myositis patients. The objective of this study is to demonstrate a relationship between race/ethnicity, sex, living in a disadvantaged neighborhood, and the frequency of being prescribed disease-specific treatment for myositis in patients seen in the rheumatology clinic.
Methods: Data from the electronic health record (EHR) of a large urban hospital were analyzed from January 1, 2010 through August 31, 2020. Independent variables included age, race/ethnicity, sex, and address with zip code. The area deprivation index (ADI) score was calculated using the neighborhood atlas website mapping tool. Rheumatologic medications were the dependent variables. Prescribed steroids, DMARDs, and cyclophosphamide were compared between socioeconomic and racial/ethnic groups. Prescription of non-steroidal medications was also compared. Regression analysis was used to predict steroid use as a function of age, race/ethnicity, sex, and ADI. The analysis was repeated for DMARD and cyclophosphamide use.
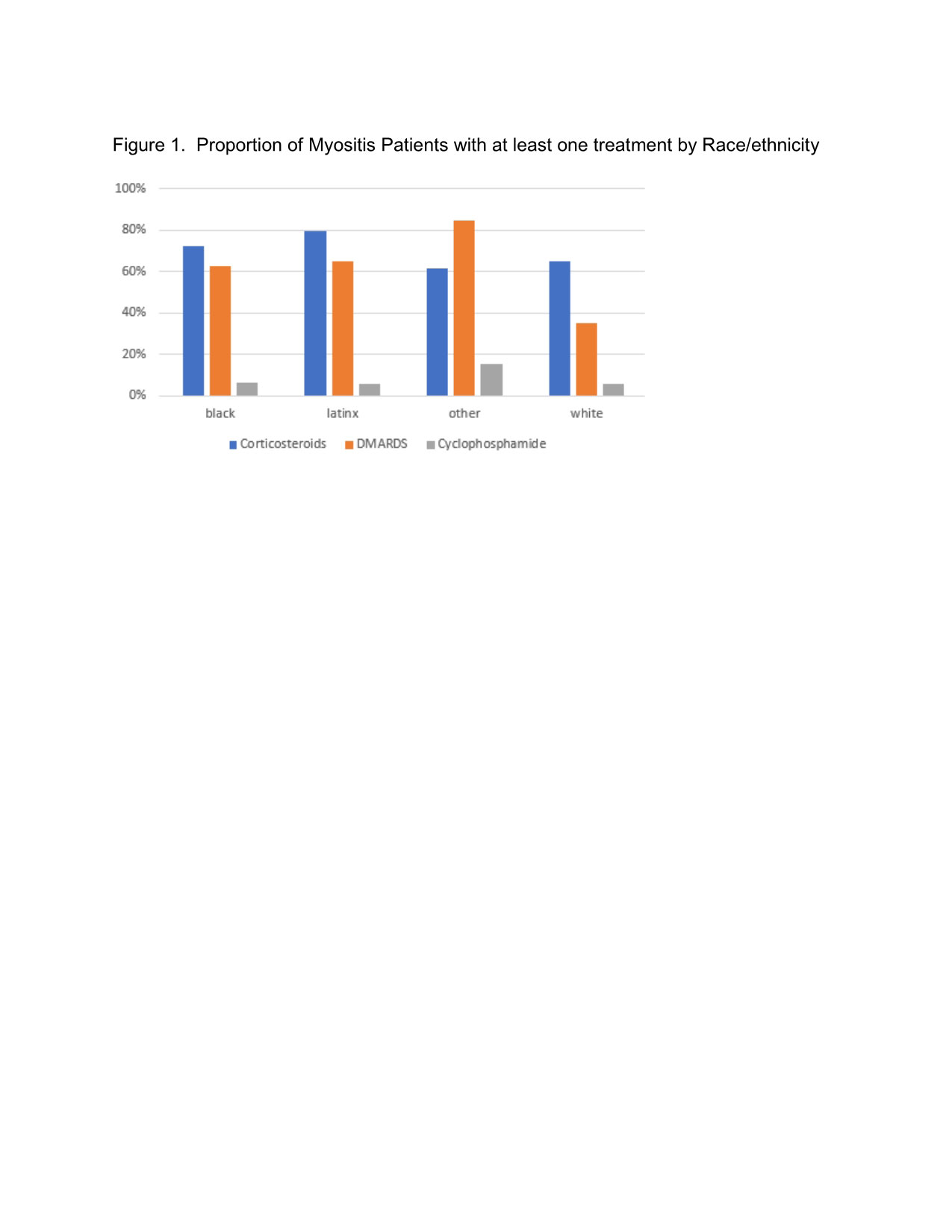
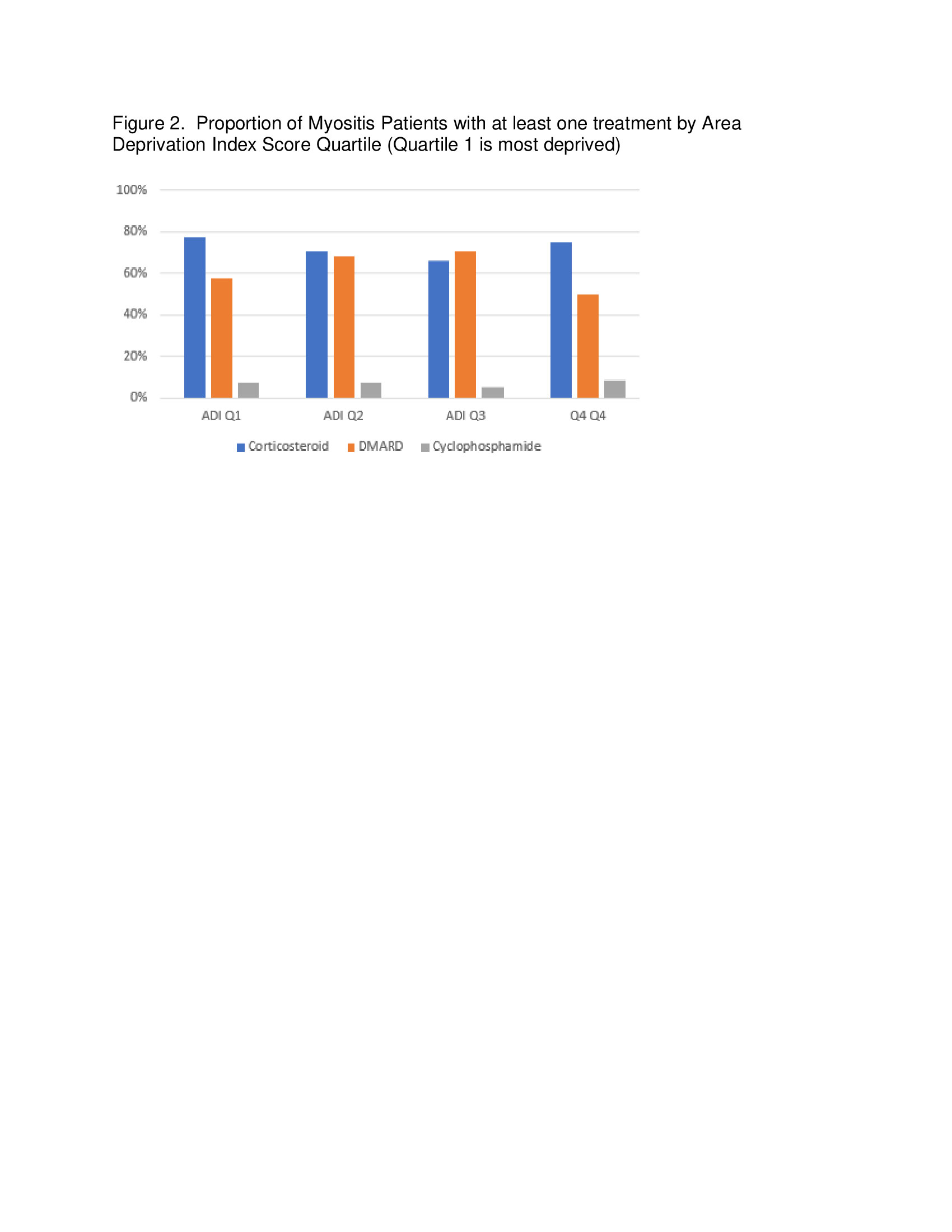
Results: There were 158 unique patients with myositis. Of these, 118 (74.7%) were women and 40 (25.3%) were men. Race/ethnicity was 17 (10.8%) non-Hispanic Whites, 94 (59.5%) non-Hispanic Blacks, 34 (21.5%) Latinx, and 13 (8.2%) Other. Women were more likely to receive cyclophosphamide, mycophenolate, or rituximab than men. Men were more likely to receive etanercept than women. ADI scores were higher among Black and Latinx patients compared with White patients (p < 0.00001). There was no difference between steroid (p=0.41) or cyclophosphamide (p=0.93) use between minority and white patients. White patients were 22.6% as likely to receive a DMARD as Black patients (p< 0.016). Latinx patients were as likely to receive a DMARD as Black patients. Results showed that physician prescribing pattern does not vary with area deprivation index scores.
Conclusion: Among patients with myositis, Blacks and Latinx are more likely to live in an area with a higher area deprivation index score. There was no difference between minorities and Whites of being prescribed a steroid or cyclophosphamide; White patients were less likely to receive a DMARD than Black patients. Physician prescribing pattern did not vary with area deprivation scores. Future studies with larger sample sizes are needed to help quantify the relationship between area deprivation score, race/ethnicity, and sex; to better understand physician prescribing patterns in patients, particularly among minority groups; and to understand how these factors may influence disease-related health outcomes in myositis.
To cite this abstract in AMA style:
Alawneh D, Chan Z, Galanter W, Berry J, Al-Awqati M, Chang H. Disparities in Prescription Medications Among Myositis Patients in a Large Urban Medical Center [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/disparities-in-prescription-medications-among-myositis-patients-in-a-large-urban-medical-center/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/disparities-in-prescription-medications-among-myositis-patients-in-a-large-urban-medical-center/