Session Information
Date: Sunday, November 8, 2015
Title: Pediatric Rheumatology – Clinical and Therapeutic Aspects Poster I: Lupus, Scleroderma, JDMS
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose:
Mixed Connective Tissue Disease (MCTD) is a rare
rheumatic disease with overlapping features from Systemic Lupus Erythematosus (SLE),
Systemic Sclerosis (SSc) and Polymyositis. Juvenile onset MCTD (JMCTD) accounts
for approximately 25% of all cases, but knowledge about disease activity and
possible organ damage after long-term disease is limited. The purpose of this
study is to describe disease activity- and damage in JMCTD after long-term
follow-up, and identify possible predictive factors for unfavourable outcome.
Methods:
A cohort of 48 patients with JMCTD from all regions of Norway was examined in a cross-sectional study. Inclusion criteria were fulfilment of the
Kasukawa- or Alarcon-Segovia criteria and symptom-onset before 18 years. All
patients were clinically examined after mean disease duration of 16.4 (SD 9.9) years. Data from the time of diagnosis were
obtained by chart reviews in 45 patients.
As there are no validated criteria for disease activity
and damage in MCTD, the following disease activity- and damage scores
attributable to SLE, SSc and Juvenile Idiopathic Arthritis (JIA) were used: Systemic
Lupus Erythematosus Disease Activity Index (SLEDAI), Rodnan skin score, Systemic
Lupus International Collaborating Clinics/ACR Damage Index (SLICC/ACR DI) and Juvenile
Arthritis Damage Index (JADI). Remission was defined as fulfilment of the
Wallace criteria for remission in JIA, plus the absence of leucopoenia,
myositis, progressive lung- or esophageal manifestations and progressive
sclerodactyly. Active disease was defined as absence of remission.
Results:
At 16 year follow-up, 31 patients (65%) were considered
to have active disease, and 17 (35%) were in remission on or off medication
(table 1).
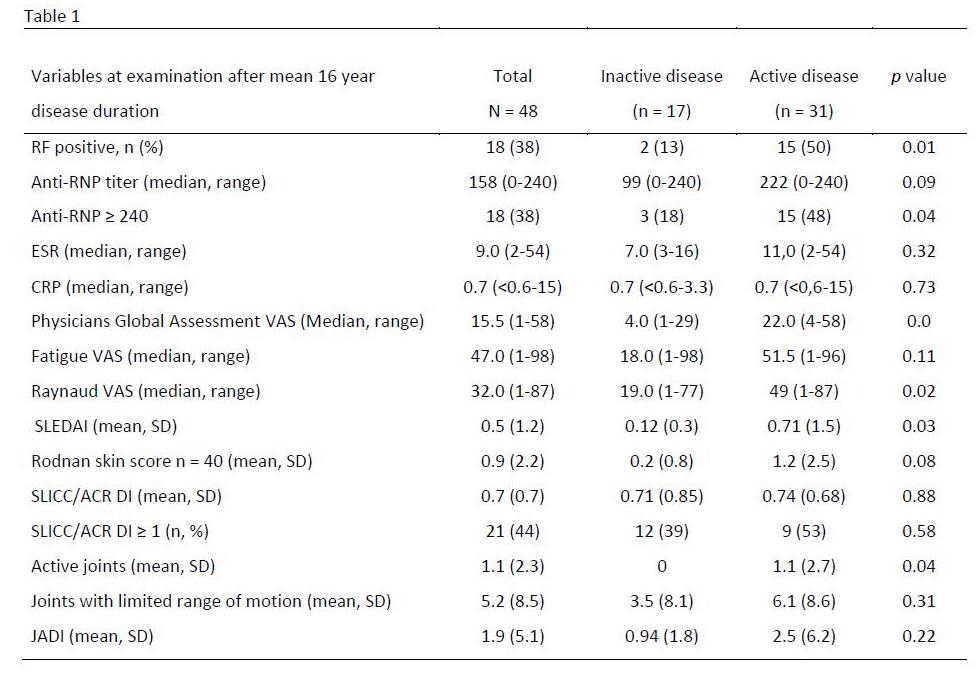
The patients with active disease had more frequently
high levels of anti-RNP and positive Rheumatoid Factor (RF) than those in
remission. Twenty one patients (44%) had a SLICC score of 1 or more. The main
reason for the high score was the large proportion with signs of pulmonary
fibrosis (21 patients, 44%), where 21 (44%) had reduced diffusion capacity or
vital capacity, and 12 patients (25%) had CT-verified pulmonal fibrosis.
Disease duration, positive RF at diagnosis and number
of months treated with prednisolone were associated with persistently active
disease after 16 years, but only the presence of positive RF at diagnosis was
identified as a predictor in the multivariate analysis at follow-up (OR 6.84,
95% CI 1.6-29.8).
Conclusion:
In this Norwegian cohort of juvenile onset MCTD, we
found that after 16 years of disease duration, 65% had ongoing active disease,
and these patients had more frequently high levels of anti-RNP and positive RF.
A large proportion of the patients had signs of disease damage with a score of
≥1 assessed with SLICC/ACR DI.
Presence of positive RF at time of diagnosis predicted
ongoing active disease.
To cite this abstract in AMA style:
Hetlevik SO, Flatø B, Rygg M, Nordal EB, Lilleby V. Disease Activity, Disease Damage and Predictive Factors in Juvenile Onset Mixed Connective Tissue Disease – a Norwegian Nationwide Study [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/disease-activity-disease-damage-and-predictive-factors-in-juvenile-onset-mixed-connective-tissue-disease-a-norwegian-nationwide-study/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/disease-activity-disease-damage-and-predictive-factors-in-juvenile-onset-mixed-connective-tissue-disease-a-norwegian-nationwide-study/