Session Information
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Primary Sjögren’s Syndrome (pSS) is characterized by xerophthalmia, xerostomia and increased lymphoma risk. To address heterogeneity in symptoms, Tarn et al. applied cluster analysis on a pSS population. They identified four subgroups based on patient-reported outcomes assessing dryness, fatigue, pain, anxiety and depression: low symptom burden (LSB), pain dominant with fatigue (PDF), dryness dominant with fatigue (DDF) and high symptom burden (HSB). These groups were considered true endotypes due to differences in hematological, biological, autoimmune and transcriptomic parameters.
Salivary gland ultrasound (SGUS) is emerging as essential tool in the evaluation of pSS, but its link to these endotypes is unknown. Therefore, we explored SGUS outcomes in relation to endotypes in patients with definite and suspected pSS.
Methods: Definite pSS patients (n=171) fulfilling the 2016 ACR/EULAR classification criteria, and suspected pSS patients (n=119), positive for at least one criterion, were included in the Belgian Sjögren’s Syndrome Transition Trial (BeSSTT). Both patient groups were stratified into endotypes using the Newcastle Sjögren’s Stratification Tool. SGUS was assessed using Hocevar score (0-48); scores ≥17 were considered positive. Categories were created with 0-14 indicating negative, 15-26 low positive and 27-48 high positive results. The dataset was randomly divided into a discovery (n=203) and replication (n=87) cohort.
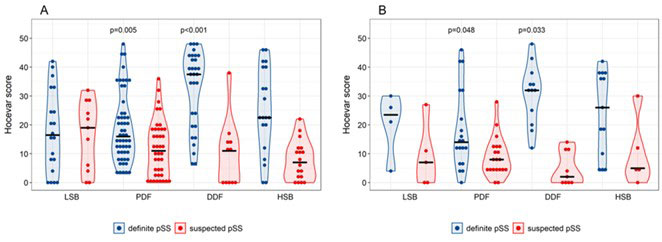
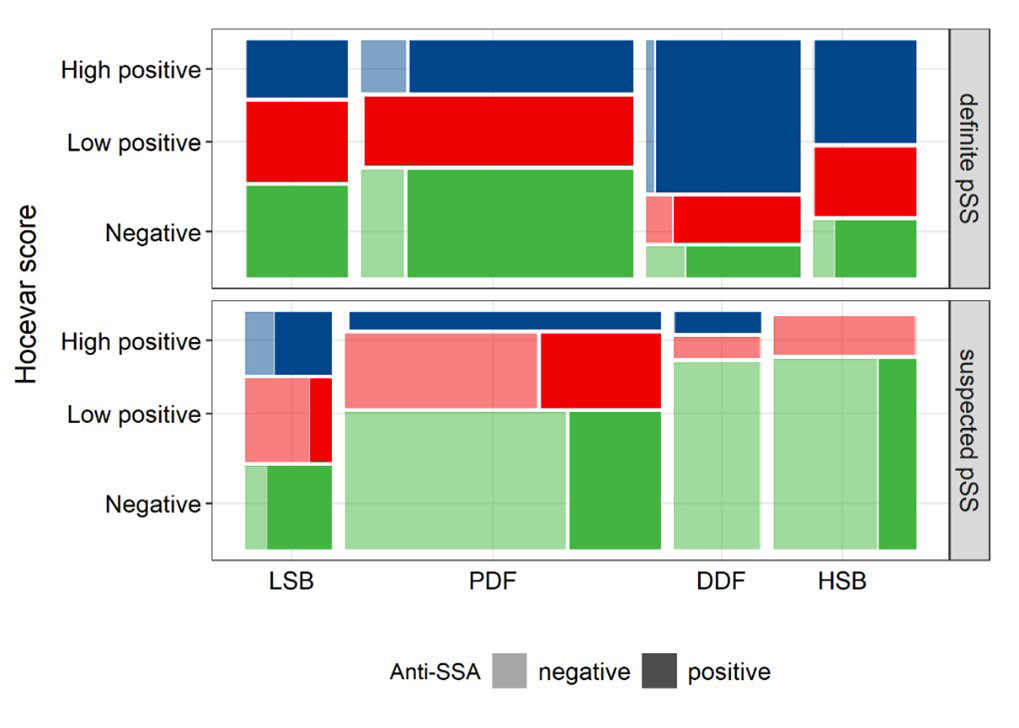
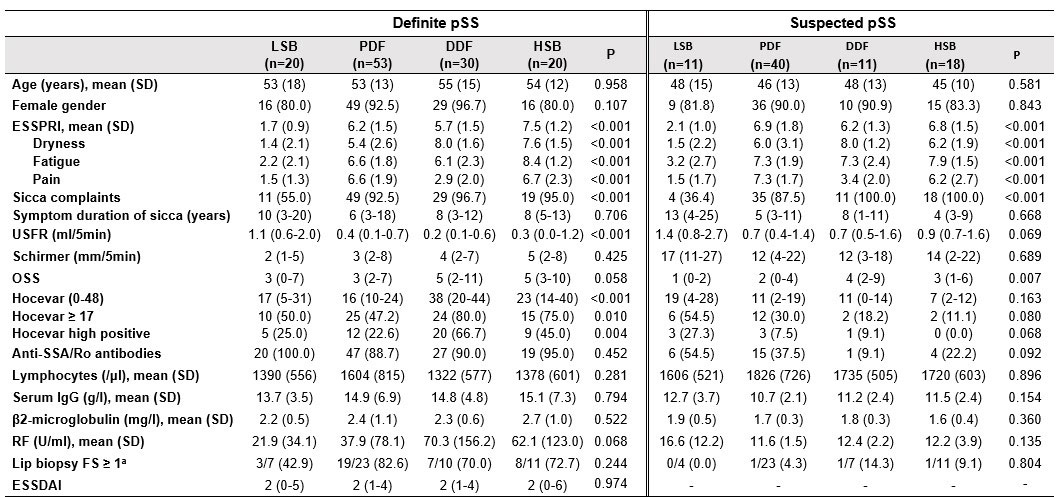
Results: In the discovery cohort, Hocevar was significantly higher amongst definite than suspected pSS patients (21 (11-36) vs 10 (2-18); p< 0.001). This was also true when comparing definite and suspected pSS subgroups within each endotype, with the exception of LSB (17 (5-31) vs 19 (4-28); p=0.823) (Figure 1). SGUS had strong discriminative power for pSS classification (AUC=0.74), especially in DDF (AUC=0.89). In definite pSS, Hocevar scores were strikingly high in DDF compared to other endotypes (38 (20-44) vs 18 (9-33); p< 0.001). Additionally, a significantly higher proportion of DDF patients had a high positive Hocevar score compared to other patients (66.7% vs 28.0%; p< 0.001) (Figure 2). Patients with high positive SGUS-scores reported a significantly higher dryness burden (p< 0.001), and had lower unstimulated salivary flow rates (p=0.005) and higher ocular staining scores (p< 0.001) than those with a negative SGUS. They had significantly lower lymphocyte counts (p=0.005), while β2-microglobuline, IgG and rheumatoid factor levels were higher (all p< 0.001), independent of endotype. Moreover, a subset of young, anti-SSA/Ro positive patients not fulfilling classification criteria showed clear SGUS abnormalities. Replication showed similar results.
Conclusion: Amongst definite pSS patients, SGUS-scores were highest in DDF compared to other endotypes, providing the first evidence of imaging abnormalities in salivary glands matching distinct biological profiles ascribed to pSS endotypes. Additionally, a subset of patients with potential early disease was detected due to presence of anti-SSA antibodies and high SGUS-scores. These results underscore the role of SGUS as powerful tool both in pSS classification and stratification.
To cite this abstract in AMA style:
Deroo L, Achten H, Genbrugge E, Bauters W, Roels D, Dochy F, Creytens D, De Craemer A, Van den bosch F, Elewaut D, peene i. Discriminative Power of Salivary Gland Ultrasound in Relation to Symptom-based Endotypes in Suspected and Definite Primary Sjögren’s Syndrome [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/discriminative-power-of-salivary-gland-ultrasound-in-relation-to-symptom-based-endotypes-in-suspected-and-definite-primary-sjogrens-syndrome/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/discriminative-power-of-salivary-gland-ultrasound-in-relation-to-symptom-based-endotypes-in-suspected-and-definite-primary-sjogrens-syndrome/