Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Symptomatic knee OA affects 14 million adults in the US. Recent estimates suggest that about 40% of people with knee OA are taking prescription opioids. Opioid use carries substantial societal costs associated with diverted opioid prescriptions and opioid use disorder (OUD), defined by the Diagnostic and Statistical Manual of Mental Disorders IV criteria for abuse and dependence. We sought to estimate the direct medical and societal cost associated with opioid consumption among patients with symptomatic knee osteoarthritis in the US.
Methods: We used a validated, widely published computer simulation model of knee OA (OAPol Model) to estimate lifetime direct medical costs associated with opioid use and the societal costs associated with opioid diversion and OUD in the US knee OA population. The direct medical costs of opioid use included the cost of medication, outpatient visits, and treatment complications including addiction and overdose. Medication, outpatient visit, and non-OUD related complication costs were derived from the 2017 Red Book, Healthcare Cost and Utilization Project, Medicare Physician Fee Schedule, and literature sources. The direct medical cost of opioid addiction and overdose was derived from published literature (Birnbaum 2011) at a per person annual cost of $16,600. Societal costs included diversion and OUD related impacts. The cost of diversion ($200/prescription) and OUD were derived from published literature (Birnbaum 2011). For those experiencing OUD, the per person cost was $17,200 for lost workplace productivity and $3,500 for criminal justice and prevention. Using data from Medicare Current Beneficiary Survey, we estimated the prevalence of opioid addiction, excluding those who overdose, among those with knee OA who had been prescribed opioids to be 0.93%. Using World Health Organization data, we estimated the prevalence of overdose to be 0.77%, resulting in a total estimated prevalence of addiction of 1.7% among knee OA opioid users. We discounted costs at 3% annually.
Results: We estimated 9 million persons have moderate or severe pain due to knee OA; the total lifetime direct medical and societal cost associated with opioid use was $14.8 billion. Direct medical costs of opioids were estimated at $897 per knee OA patient with moderate or severe pain. Societal costs per knee OA patient with moderate or severe pain were estimated at $283 for lost workplace productivity and $465 for diversion/criminal justice/prevention costs. Direct medical costs make up 55% ($8.1 billion) of the total direct medical and societal cost of opioid use in this population (Figure). The societal costs of opioid use due to lost workplace productivity costs make up 17 % ($2.6 billion) of the total cost of opioid use in this population, and diversion/criminal justice/prevention costs 28% ($4.2 billion).
Conclusion: The total direct medical and societal cost of strong opioid use in the US knee OA population is substantial. This could be due in part to the high prevalence of symptomatic knee OA in the US. Close to 50% of the total costs attributed to opioid use in this population is spent on diversion, criminal justice, prevention and work-related expenditures.
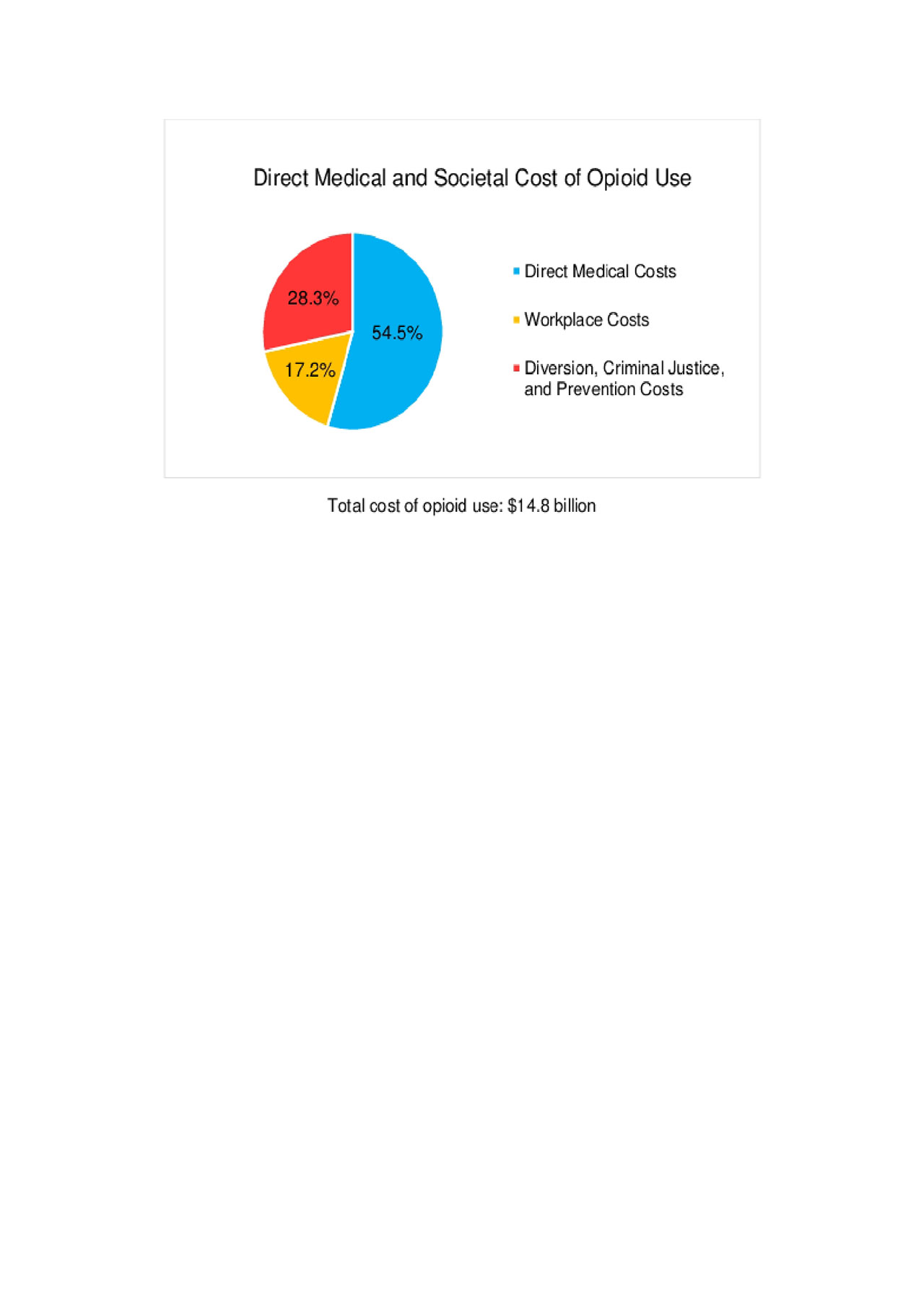
ACR2019_CostOfOpioidUse_figure
To cite this abstract in AMA style:
Huizinga J, Stanley E, Song S, Sullivan J, Katz J, Losina E. Direct Medical and Societal Cost of Opioid Use in Symptomatic Knee Osteoarthritis Patients in the United States [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/direct-medical-and-societal-cost-of-opioid-use-in-symptomatic-knee-osteoarthritis-patients-in-the-united-states/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/direct-medical-and-societal-cost-of-opioid-use-in-symptomatic-knee-osteoarthritis-patients-in-the-united-states/