Session Information
Date: Sunday, November 17, 2024
Title: RA – Treatment Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Over the past decades, the treatment of Rheumatoid Arthritis (RA) has significantly improved, making accessible therapeutic goals such as clinical and structural remission. However, a substantial number of patients show resistance to several drugs. These patients have been recently included in the definition of Difficult-to-treat (D2T) patients (1). As a new definition, research is now focusing on determining which factors may influence the resistance to multiple mechanisms of action, including patients’ intrinsic characteristics.
To identify any baseline clinical features and disease characteristics associated with a D2T phenotype in a large cohort of early RA (ERA). Moreover, in a five-year follow-up, we compared the disease and treatment-related comorbidities between the D2T and the non-D2T cohorts.
Methods: We performed a retrospective analysis recording clinical and laboratory data (TJC, SJC, C-Reactive Protein), patients-reported outcome (VAS, HAQ), and disease activity composite indexes (DAS28, SDAI, CDAI). Clinical data were collected for each ERA patient naïve to DMARD and fulfilling the ACR/EULAR 2010 classification criteria at baseline and after 6, 12, 36, and 60 months. D2T and non-D2T cohort features were compared. A logistic multivariate regression analysis was performed to confirm discriminant variables in the univariate analysis.
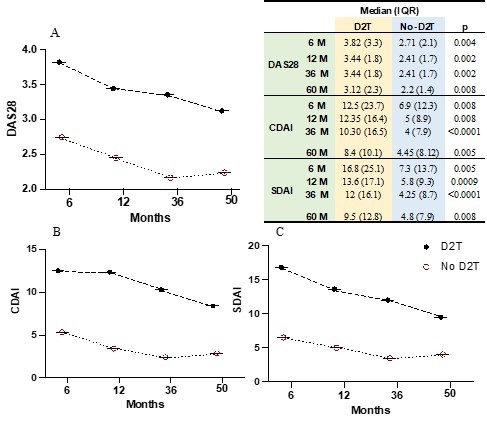
Results: We included 391 ERA patients [F/M 109/282, median age 48.2 years IQR (21.26)]; In a five-year follow-up, 42 patients matched the definition of D2T. When comparing D2T and non-D2T patients (Table 1A) the formers were characterized by a higher seropositivity rate for Rheumatoid Factor and ACPA (82.9% versus 63.6%; p=0.01 and 85.4% versus % 66.4; p=0.01), significantly higher baseline bone erosions (70.7% versus % 46; p=0.003) and higher baseline disease activity assessed with SDAI [31.7 (IQR 30.2) versus 24.7 (IQR 19.8); p=0.02] and CDAI [27.8 (IQR 27.2) versus 22.15 (IQR 17.9); p=0.04]. No other baseline features differed between the two groups for all the items (TJC, SJC, DAS28, SDAI, and CDAI, CRP) except for TJC44 [12 (17.25) versus 10(12); p=0.02] (Table 1). Discriminant variables were included in a multivariate logistic regression analysis. Baseline erosions (Y/N) were confirmed as independent predictors of evolution toward a D2T phenotype [OR 2.2 (CI 1.04 – 5.2); p=0.04]. During the follow-up, disease activity (DAS28, CDAI, SDAI) was consistently higher in the D2T group (Figure 1A-C) during all the observation time. After five years of follow-up (Table 1B), D2T patients more commonly suffered from infections (51.2% versus 27.5%; p=0.0015), and osteoporosis (25% versus 8.1%; p=0.005) and were exposed to a higher cumulative dose of glucocorticoids > 1 gram (52.5% versus 35.5%; p=0.035).
Conclusion: Our results suggest that patients characterized by baseline disease features including seropositivity (RF and/or ACPA), baseline bone erosions, and disease activity are more prone to evolve into a D2T-RA. In a five-year follow-up, D2T patients received higher GC doses and more commonly developed diseases and iatrogenic-related comorbidities such as osteoporosis and infections.
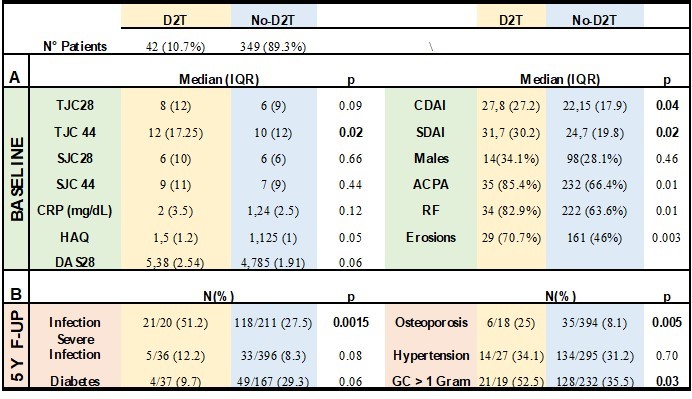
Legend: TJC28/44= Tender Joint Count 28/44; SJC28/44= Swollen Joint Count 28/44; CRP= C-Reactive Protein; HAQ=Health Assessment Questionnaire; DAS28=Disease Activity Score 28; CDAI= Clinical Disease Activity Index; SDAI= Serological Disease Activity Index; ACPA= anti-Citrullinated Protein Antibodies; RF= Rheumatoid Factor
To cite this abstract in AMA style:
Francesco N, triaille C, Emilie S, Stéphanie D, Cécile V, Stéphanie d, Tatiana S, Aleksandra A, Patrick D. Difficult to Treat Rheumatoid Arthritis Incidence and Risk Factors in the Early Arthritis UCLouvain Brussels Cohort [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/difficult-to-treat-rheumatoid-arthritis-incidence-and-risk-factors-in-the-early-arthritis-uclouvain-brussels-cohort/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/difficult-to-treat-rheumatoid-arthritis-incidence-and-risk-factors-in-the-early-arthritis-uclouvain-brussels-cohort/