Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
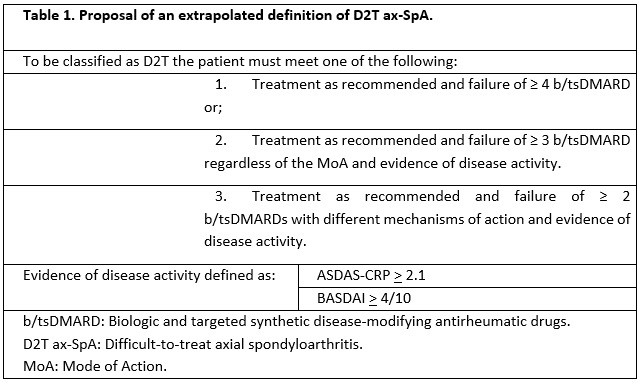
Background/Purpose: The term “Difficult-to-Treat” (D2T) defines those patients who remain active despite having undergone various treatments within the established recommendations. This concept is defined by EULAR for rheumatoid arthritis (RA)1, and is yet to be presented in axial spondyloarthritis (ax-SpA) by the ASAS group, although it is proposed by some studies as those who require three or more biological drugs2.
Our objectives are to determine the prevalence of D2T-ax-SpA in our Spondyloarthritis hospital registry cohort and to determine predictive factors prior to first b/ts DMARD in D2T-ax-SpA patients.
Methods: Single-center, retrospective study using a longitudinal cohort of patients with ax-SpA from a third level hospital registry in Cataluña who met the criteria for axial spondyloarthritis according to ASAS, from January 2000 to September 2022 and had a follow-up of more than 6 months with valid baseline information.
Sociodemographic, clinical, radiographic and treatment variables were collected. Patients in our study were classified as D2T according to a series of variables to achieve the most specific definition (Table 1). The comparator group included patients with axial spondyloarthritis with use of at least one b/tsDMARDs and who did not meet our D2T criteria.
For the bivariate analysis, the categorical variables were analyzed using the chi-square test and Fisher’s test, the quantitative variables through the student’s t test and U Mann Whitney.
For the multivariate analysis, we used logistic regression using imputations of missing values through a multiple imputation by chained equations.
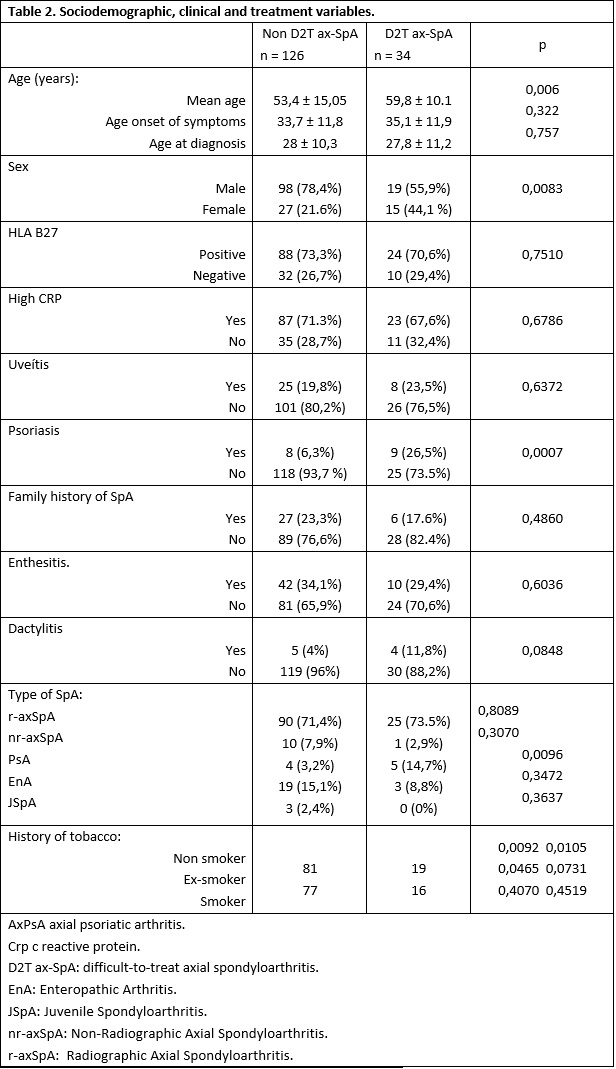
Results: Five hundred and ten patients met the ASAS criteria for the diagnosis of AxSpA, 161 of whom had received treatment with at least one ts/bDMARD. Thirty-four (21.12%) met our definition of D2T, of which 55.9% were men, mean age 59.82 years (+/- 10.13).
No significant differences were found in the presence of comorbidities such as arterial hypertension, hyperlipidemia, diabetes mellitus, ischemic heart disease, and cerebrovascular disease. Nor in disease activity index or clinical manifestations such as uveitis, inflammatory bowel disease, enthesitis, arthritis, dactylitis. These results are summarized in Table 2.
Female sex (p= 0.0083), presence of psoriasis (p= 0.0007), onset as psoriatic axial spondyloarthritis (p= 0.0096) were found as risk factors for D2T AxSpA (Table 2). These findings were confirmed in the multivariate analysis (Table 3).
We also found a tendency to greater cervical involvement (SASSSmCC p= 0.025; BASRI CC p= 0.069; FLECHE p= 0.061), and being an active smoker in these patients, although this could not be demonstrated in the multivariate analysis.
Conclusion: Female sex, presence of psoriasis, onset as psoriatic axial spondyloarthritis prior to bDMARD seem to act as risk factors for D2T AxSpA.
References: 1.Nagy G, Roodenrijs NMT, Welsing PM, et al. (2021) EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis 80 (1):31-5 2. Wendling D, Verhoeven F, Prati C (2022) Is the Difficult-to-Treat (D2T) concept applicable to axial spondyloarthritis? Joint Bone Spine 90 (3):105512

To cite this abstract in AMA style:
MONTERO F, Berbel Arcobé L, Carpio Astudillo K, Bellón J, Juanola Roura X. Difficult to Treat Axial Spondyloarthritis. Predictors of Poor Outcomes [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/difficult-to-treat-axial-spondyloarthritis-predictors-of-poor-outcomes/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/difficult-to-treat-axial-spondyloarthritis-predictors-of-poor-outcomes/