Session Information
Date: Sunday, November 7, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster II: Miscellaneous Aspects of RA (0786–0812)
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: Methotrexate (MTX) is often the primary medication to treat various rheumatic diseases, including rheumatoid arthritis, psoriasic arthritis and many other inflammatory diseases. MTX is significantly less expensive than other alternatives and has been shown in randomized controlled trials to be effective in controlling disease activity, enhancing patient quality of life, and potentially decreasing mortality among patients with inflammatory disorders. Despite its advantages, however, a major concern has been the potential for hepatic fibrosis associated with long term MTX usage.
The present study investigates the association between cumulative MTX intake and development of liver fibrosis among patients with rheumatic diseases. We utilized non-invasive transient elastography (FibroScan) to assess for liver fibrosis among patients in a large academic outpatient rheumatology clinic.
Methods: All patients with inflammatory arthritis treated with MTX were offered screening with FibroScan. All patients who volunteered to participate were included. A certified FibroScan technician measured the liver stiffness after patients adhered to a minimal 90-minute fast. Health and medication information were collected from the patient. FibroScan measurements were recorded as both numerical values represented by the machine in kilopascal (kPa), as well as an ordinal classification from F0 (normal liver stiffness) to F4 (cirrhosis).
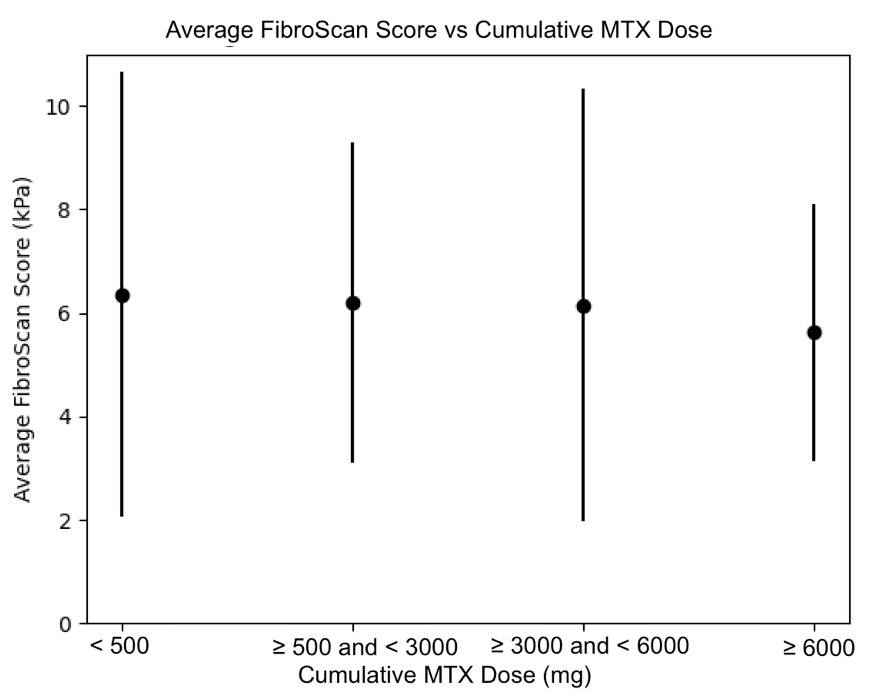
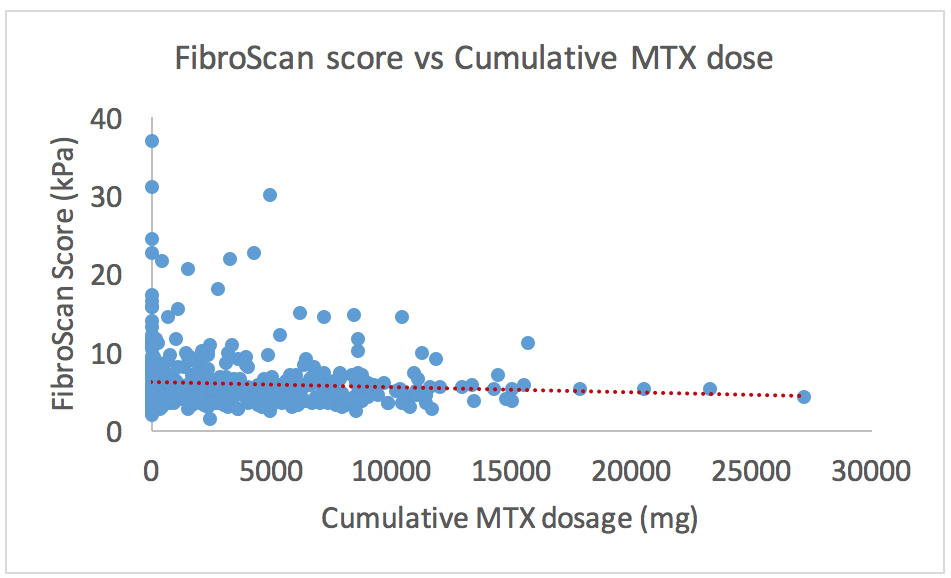
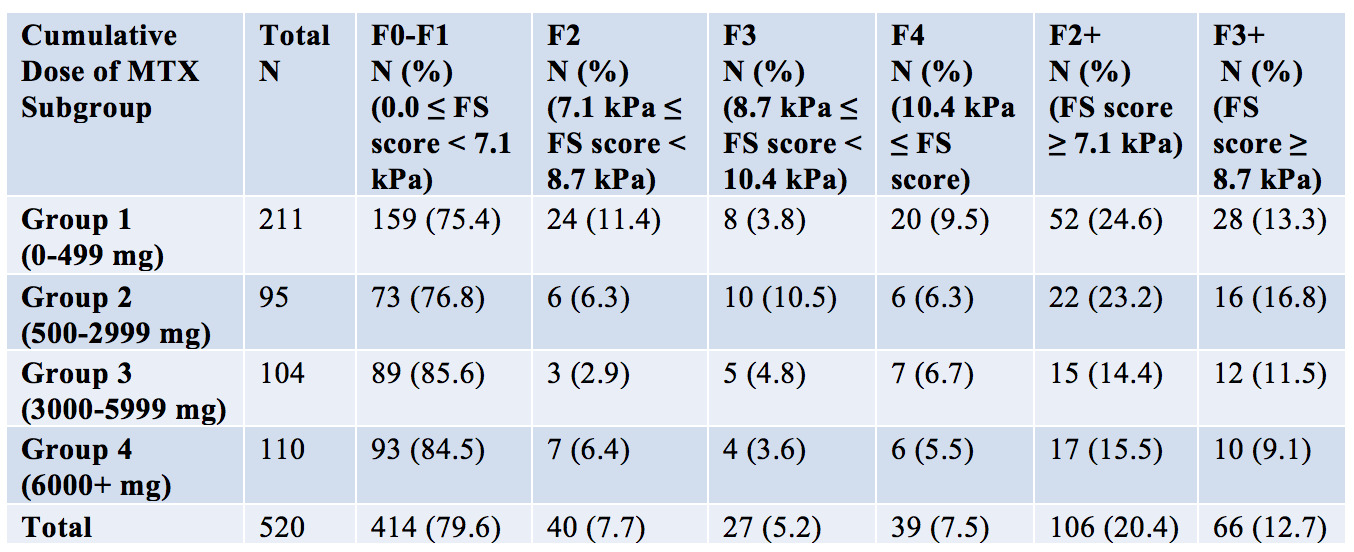
Results: Five hundred and twenty rheumatologic patients were included in the primary analysis. FibroScan scores ranged between 1.5 kPa and 37.1 kPa, with an average of 6.13 kPa ± 3.76 kPa. Univariate and multivariate linear and logistic regression models were used for analysis in this study. In multivariable linear regression analysis, statistically significant factors were BMI (regression coefficients: 0.060, p=0.001), waist circumference (0.041, p=0.015), male sex (0.109, p=0.004), and age (0.026, p=0.054). The population was then divided into quartiles based on the participant’s cumulative dosage of MTX. The prevalence of F3/F4 liver fibrosis (i.e. FS ≥ 8.7 kPa) was 13.3% in the control group (MTX cumulative dosage < 500mg), 9.1% in subgroup 4 (MTX >6000mg) and 12.7% in the entire sample. Compared with subgroup 1 (control), MTX subgroups 2-4 were not significantly correlated with higher FS scores (p-values 0.82, 0.59, and 0.18 respectively).
Conclusion: FibroScan scores compatible with liver fibrosis were seen in all MTX subgroups; however, no significant correlation between the cumulative MTX dosage and liver stiffness was observed, even at high MTX doses. The analysis showed significant correlations between the FibroScan score and BMI, waist circumference, male sex, and age. Further studies are needed to assess agreement between liver function tests and FibroScan scores and to better identify threshold FibroScan scores warranting methotrexate discontinuation, particularly in patients with additional risk factors such as high BMI and waist circumference.
To cite this abstract in AMA style:
Darabian S, Wade j, Wade S, Kur J, Badii M. Diagnostic Utility of FibroScan in Screening for Liver Injury in Patients with Inflammatory Arthritis on Treatment with Methotrexate (MTX) [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/diagnostic-utility-of-fibroscan-in-screening-for-liver-injury-in-patients-with-inflammatory-arthritis-on-treatment-with-methotrexate-mtx/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/diagnostic-utility-of-fibroscan-in-screening-for-liver-injury-in-patients-with-inflammatory-arthritis-on-treatment-with-methotrexate-mtx/