Session Information
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Enthesitis is a key domain in psoriatic arthritis (PsA). The Diagnostic Ultrasound Enthesitis Tool (DUET) study aims to develop a new PsA-specific sonographic scoring system for enthesitis, to assist with the diagnosis of PsA. We present a preliminary analysis examining the distribution of elementary ultrasound lesions in PsA and controls.
Methods: The DUET study prospectively enrolled patients with early PsA, psoriasis alone, and non-psoriatic controls in 17 centers. Participants underwent a standardized ultrasound exam protocol of 16 entheseal sites in the upper and lower extremities by local site sonographers. Subsequently, scans were evaluated by three central readers to derive a consensus score. Abnormalities were scored on a semi-quantitative scale for Inflammatory lesions: hypoechogenicity (0-1), thickening (0-1), Power Doppler (PD, 0-3); and Structural lesions: calcification (0-3), enthesophyte (0-3), Erosion (0-1). The differences in the distribution of lesions between PsA and controls were assessed using trend test.
Results: We analyzed 213 patients with PsA (mean age 49.4±13.9, 51.2% female) and 106 controls (mean age 49.2±15.5, 58.5% female). The mean duration of PsA was 1.9±3.4. None of the participants received biologic/targeted-synthetic DMARD. Notably, 70% of PsA patients and 49% of controls exhibited tenderness in at least one enthesis.
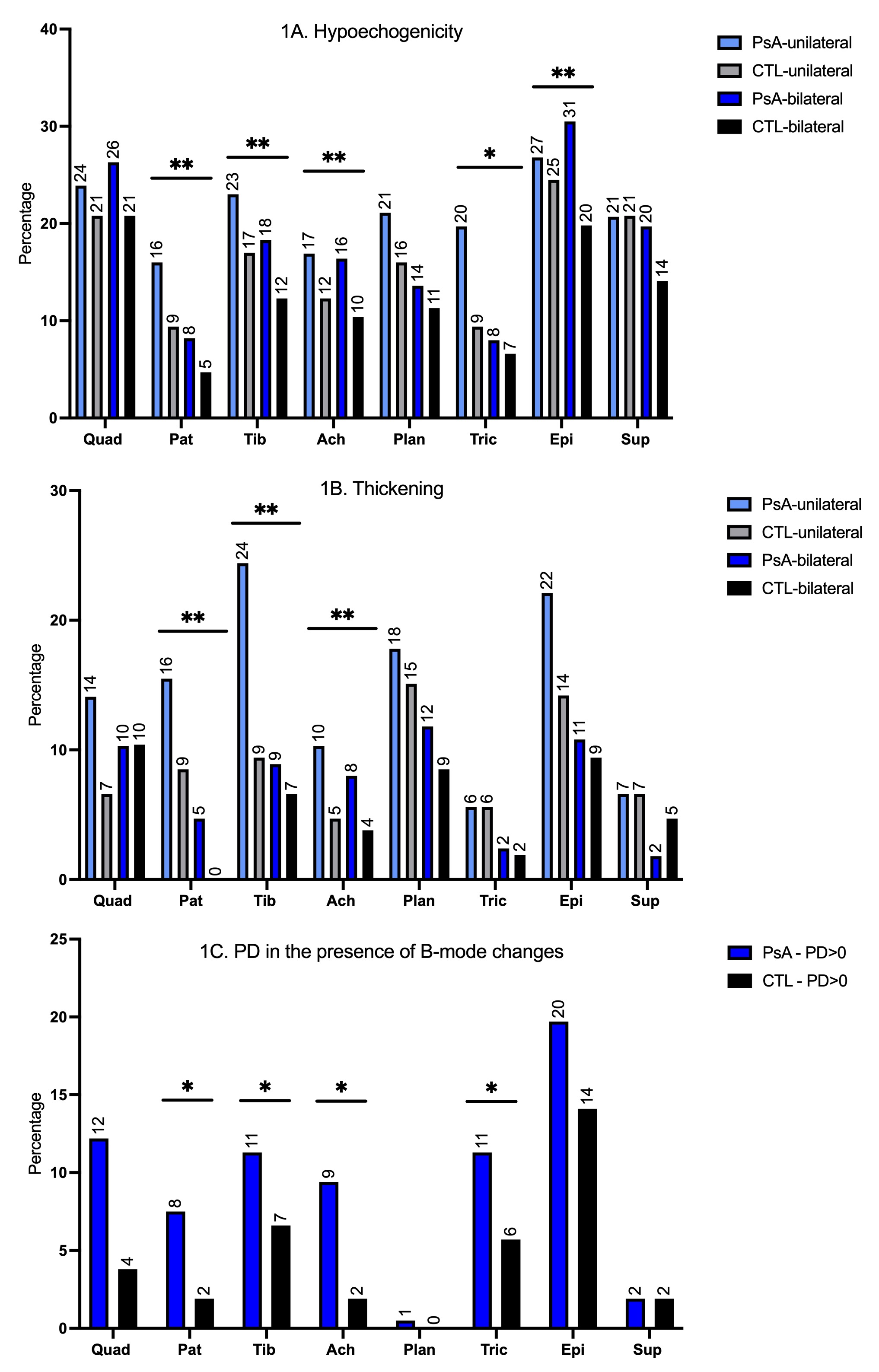
While the prevalence of inflammatory elementary lesions was generally higher in PsA than in the controls, the variations across the two groups depended on the specific entheseal site (Figure 1). Particularly, pronounced differences were observed in the patellar tendon insertions to the patella and tibial tuberosity, Achilles and triceps tendon.
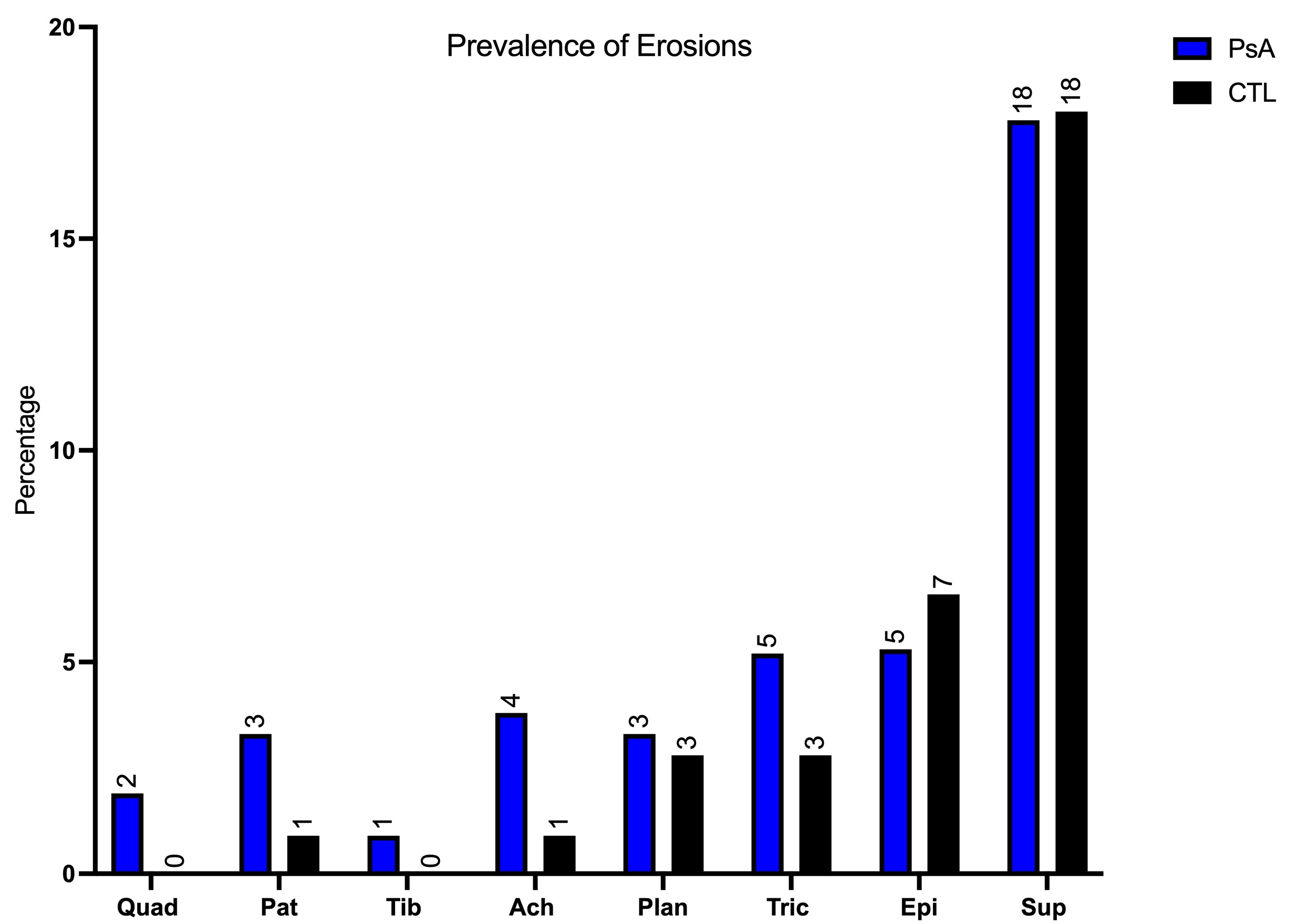
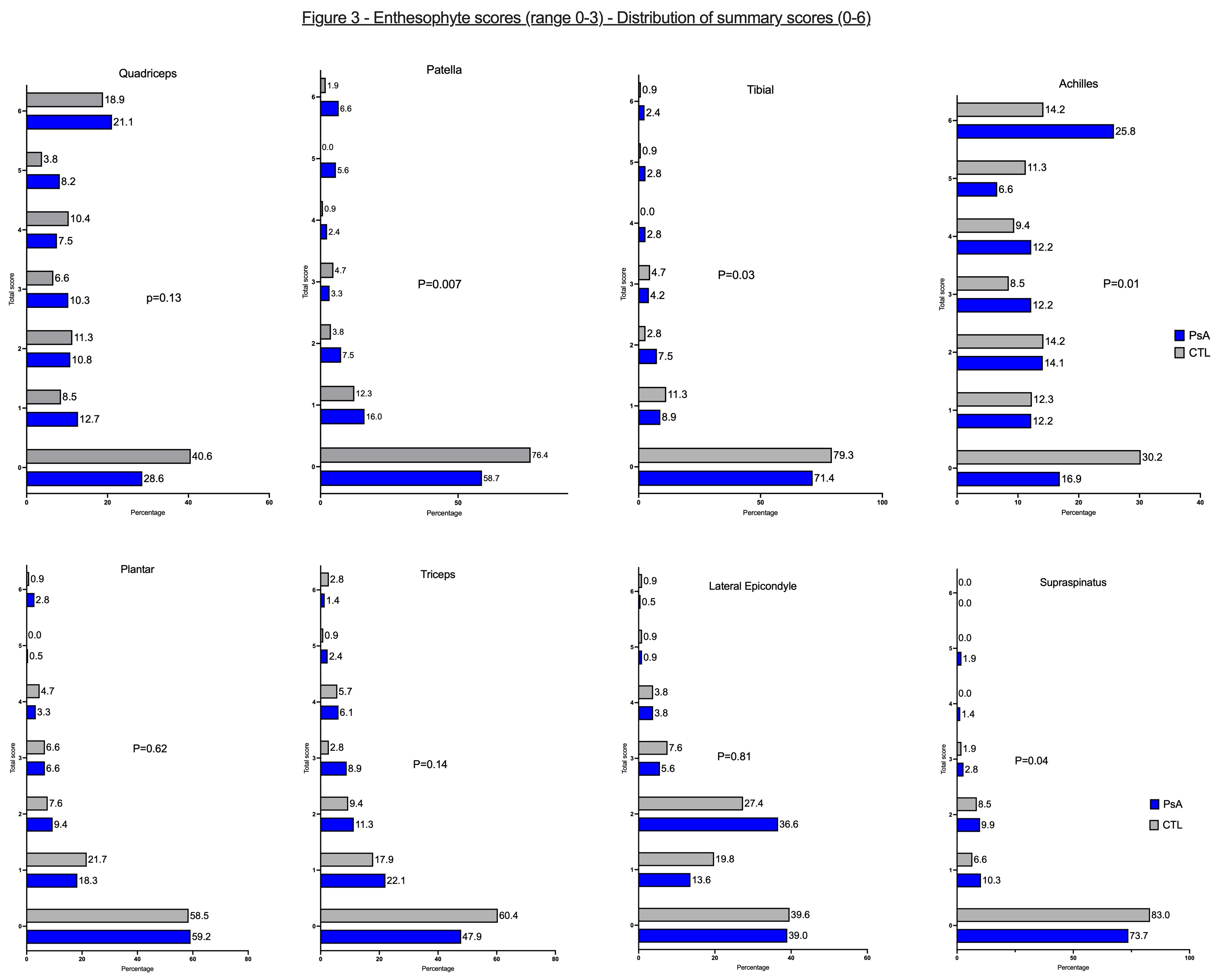
While generally infrequent, PD signal was notably higher in PsA patients, especially if detected in the presence of hypoechogenicity or thickening. Bone erosions were rare across most sites (Figure 2) and predominantly found in PsA cases. Exceptions are the supraspinatus insertions and lateral epicondyles, where erosions were more frequent, however comparable in PsA and controls. Enthesophytes were common in both PsA patients and controls, however, PsA patients had larger enthesophytes at the patellar tendon origins and insertions, Achilles, and supraspinatus than controls (Figure 3).
Conclusion: Sonographic entheseal abnormalities are not exclusive to PsA. Therefore, to distinguish PsA from controls, any sonographic scoring system should account not only for the presence of particular lesions but also for their severity and the precise entheseal site affected. This preliminary analysis will inform the next steps of developing a composite ultrasound score aimed at aiding in the diagnosis of PsA.
To cite this abstract in AMA style:
Eder L, Acayaba de Toledo R, Afgani F, Bakewell C, Carron P, Elnady B, Haddad A, Kavanaugh A, Katz A, Kohler M, marin j, Adrien N, Rosemffet M, Polachek A, Rodriguez E, Szentpétery Á, Singh A, Stoenoiu M, Tinazzi I, Yinh J, Kaeley G, Aydin S. Diagnostic Ultrasound Enthesitis Tool (DUET) for Psoriatic Arthritis: The Distribution of Elementary Lesions Is Influenced by Site [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/diagnostic-ultrasound-enthesitis-tool-duet-for-psoriatic-arthritis-the-distribution-of-elementary-lesions-is-influenced-by-site/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/diagnostic-ultrasound-enthesitis-tool-duet-for-psoriatic-arthritis-the-distribution-of-elementary-lesions-is-influenced-by-site/