Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
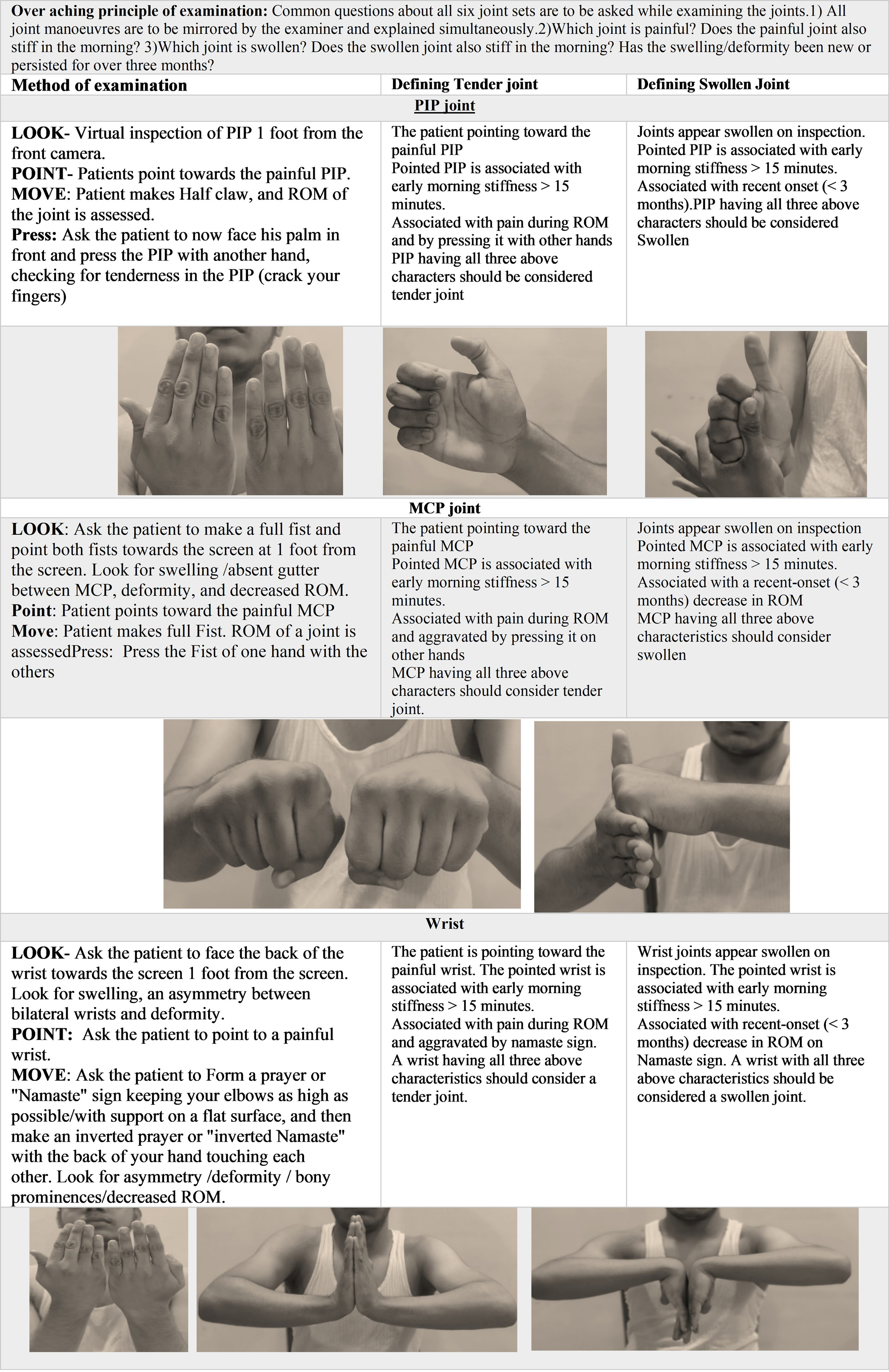
Background/Purpose: The rapid adaptation of telemedicine in rheumatology practice brings standardization, reliability and legality challenges. Therefore, it is necessary to develop dependable virtual instruments for the accurate assessment of patients, which are comparable to the standard face-to-face examination. We have developed a virtual musculoskeletal examination, and this communication highlights its usefulness in assessing the disease activity in patients with rheumatoid arthritis (RA).
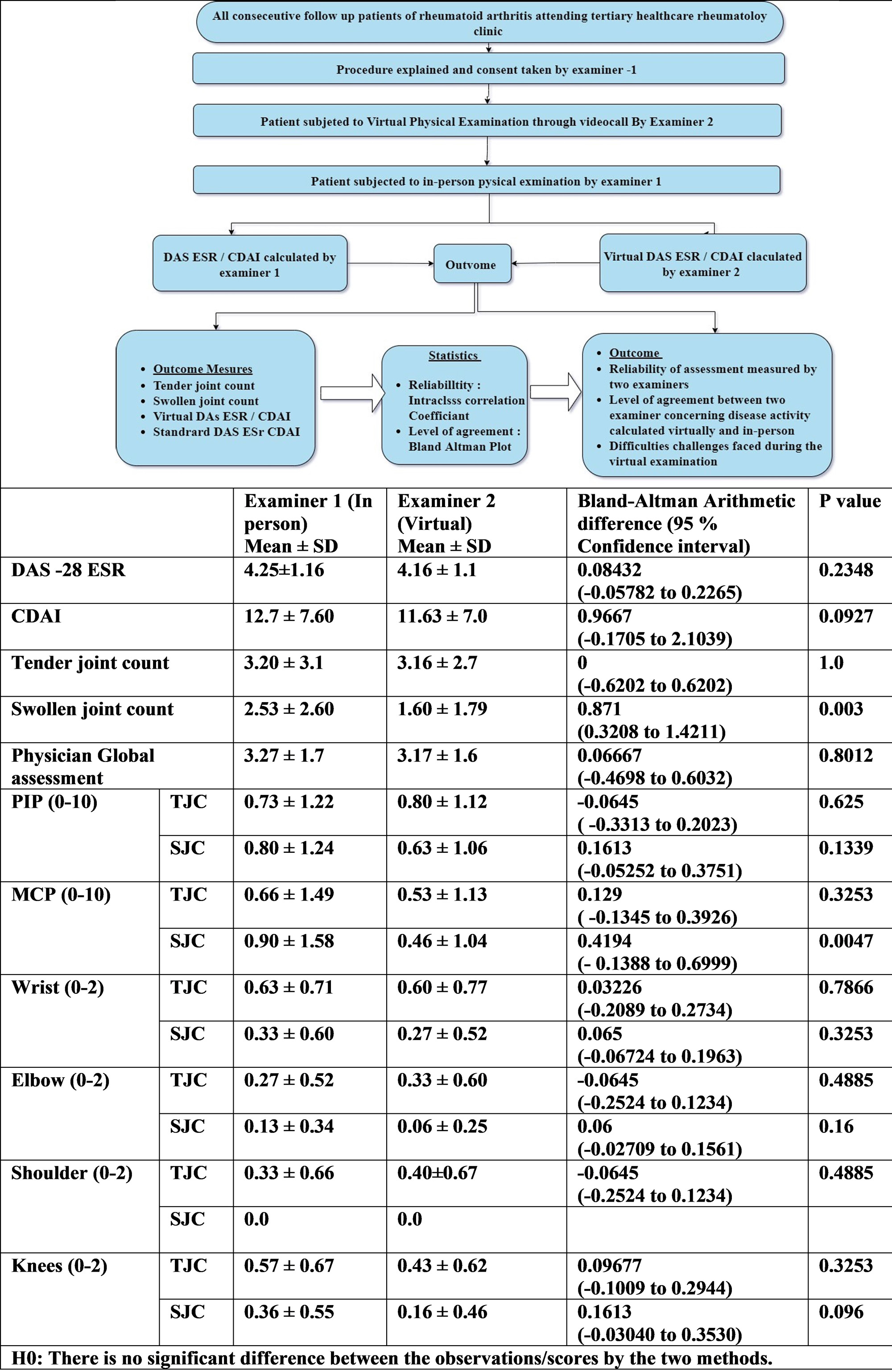
Methods: Thirty follow-up patients with RA (29 women) attending the rheumatology OPD clinic of a tertiary care hospital were recruited over a month. Disease activity was independently assessed using a novel virtual MSK (Virtual DAS 28 ESR/CDAI) examination method (Table 1 and 2) and a standard in-person method (DAS 28 ESR/CDAI) by two different examiners blinded to each other’s results. (Table 3)To determine test-retest reliability, we used intra-class correlation coefficients, and for the degree of agreement, we used Bland-Altman plots
Results: The reliability of assessments between the two examiners, as judged by inter-class correlation, was excellent for Diease Activity Score of RA (DAS–28 ESR) and Clinical Disease Activity Index (CDAI) (ICC > 0.9), good for the total tender joint count and swollen joint count (ICC 0.75-0.91), and moderate for global physician assessment (0.50-0.75). (Table 3) Thus, the observations of two examiners to calculate disease activity using virtual and standard methods are reliable and reproducible across all measurements, based on an excellent intraclass correlation coefficient. The level of agreement tested using a Bland Altman plot showed that the mean absolute difference (bias) between Virtual DAS ESR 28 and DAS 28 ESR was 0.084 (% 95 CI -0.05782 to 0.2265) with p = 0.2348, which was well below the minimal clinically important difference (MCID) for DAS-ESR, which was 1.2, suggesting an acceptable level of agreement. Similarly, the mean absolute difference (bias) between the Clinical disease activity index (CDAI) and Virtual CDAI was 0.9667 (% 95 CI-0.1705 to 2.1039) with P=0.0927, which was well below the MCID for CDAI, which is 12, suggesting an acceptable level of agreement. There was a significant difference in the level of agreement concerning the total number of swollen joints counted. Thus ,there was an acceptable level of agreement between the two examiners in calculating disease activity virtually and in person using the novel MSK examination method.
Conclusion: Our novel virtual MSK test is consistent and comparable to the in-person assessment of follow-up patients in rheumatoid arthritis with regard to the measurement of disease activity. Although there was some variability in the number of swollen joints, the new approach showed good reliability and an acceptable level of agreement. It is pragmatic, and we recommend its further refinement for routine use in tele-consultancy.

To cite this abstract in AMA style:
Yadav S, Shaikh A, Balakrishnan C. Development and Validation of a Virtual Musculoskeletal Examination Method for Disease Activity Assessment in Rheumatoid Arthritis Patients [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/development-and-validation-of-a-virtual-musculoskeletal-examination-method-for-disease-activity-assessment-in-rheumatoid-arthritis-patients/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/development-and-validation-of-a-virtual-musculoskeletal-examination-method-for-disease-activity-assessment-in-rheumatoid-arthritis-patients/