Session Information
Date: Monday, November 14, 2016
Title: Rheumatoid Arthritis – Clinical Aspects - Poster II: Co-morbidities and Complications
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Rheumatoid arthritis (RA) is associated with increased cardiovascular morbidity and mortality. This cardiovascular risk is mainly determined by the lipid profile, which may change during the course of the disease(1). For a proper cardiovascular risk assessment stable lipid values should be used and in cardiovascular risk prediction models mostly lipid ratios are applied. As the increased cardiovascular risk is already present at the time of diagnosis, it is important to initiate cardiovascular risk management as early as possible in the disease(2). However, first it is necessary to know if measurement of the lipid profile is adequate (i.e. stable lipid values) early in the disease. The aim of this study was to 1) investigate the change in lipid profile during the first 4 weeks of RA treatment 2) analyse the association between the alteration in the lipid profile and the change in ESR.
Methods: In 66 consecutive DMARD-naive early RA patients lipid profile and disease activity were measured. This was repeated after four weeks of treatment with methotrexate (3 weeks 10 mg, 4th week 17.5 mg) and prednisolone (30 mg tapered to 10 mg). Lipid profile assessment comprised TC, HDL-C, LDL-C, triglycerides and apolipoprotein A and B (Apo A and Apo B). Disease activity was assessed by the disease activity score of 44 joints (DAS44), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Patients on statins were excluded. The change in lipid profile (week 4 minus week 0) versus change in ESR was analysed in 2 patient groups: a group with high (median -31.0 mm/h) and a group with low (median -3.0 mm/h) improvement in ESR.
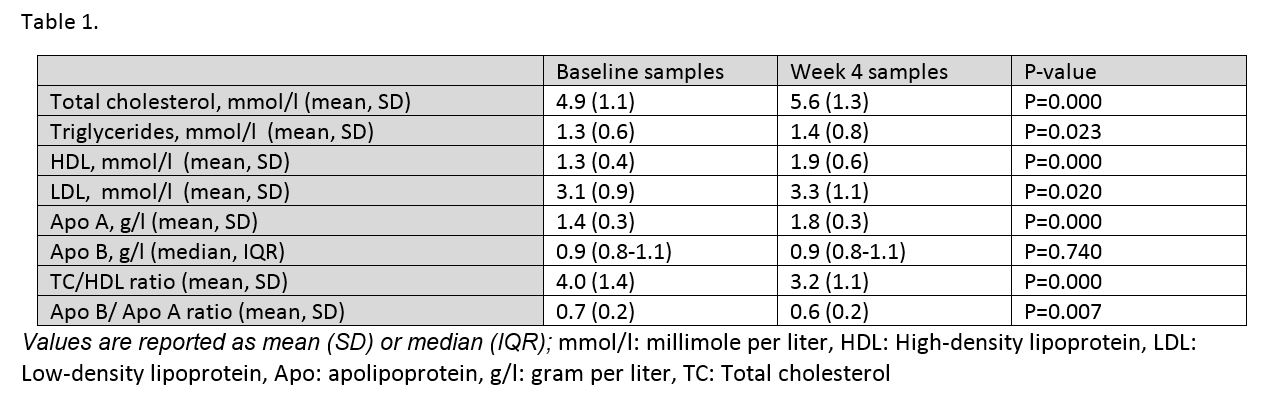
Results: Three patients on statins were excluded, analyses were thus performed on 63 early RA patients. All components of the lipid profile increased significantly during treatment, except for Apo B. In addition, ratios of lipid values, particularly the TC/HDL cholesterol ratio improved significantly (table 1). The group with high ESR versus the group with low ESR improvement had a significantly higher increase in TC, HDL-C, LDL-C and Apo A levels. This was 2.7% in the group with less improvement in ESR and 23.1% in the most improvement group. The spearman rho test showed a correlation between delta ESR and delta TC, HDL, LDL and Apo A of r=0.456, r=0.313, r=0.507 and r=0.281, respectively (all p<0.05).
Conclusion: Lipid levels increased significantly after four weeks of methotrexate and prednisolone treatment after RA diagnosis and this change is associated with the improvement in ESR. In both groups ratios of lipid values improved substantially. Hence, cardiovascular risk management in early arthritis should be postponed until low disease activity has been obtained, as assessment during active disease leads to an inappropriately high cardiovascular risk estimation. References: 1) Nat Rev Rheumatol 2013 Sep;9(9):513-23. 2) Arthritis Res Ther 2010;12(4):R158.
To cite this abstract in AMA style:
Turk SA, van Schaardenburg D, Lems WF, Nurmohamed MT. Determination of the Lipid Profile in Active Disease Leads to Incorrect Cardiovascular Risk Prediction in Early Rheumatoid Arthritis Patients [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/determination-of-the-lipid-profile-in-active-disease-leads-to-incorrect-cardiovascular-risk-prediction-in-early-rheumatoid-arthritis-patients/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/determination-of-the-lipid-profile-in-active-disease-leads-to-incorrect-cardiovascular-risk-prediction-in-early-rheumatoid-arthritis-patients/