Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Early initiation of DMARDs and targeted therapy to achieve remission are said to offer the best opportunity to prevent radiographic damage in early inflammatory arthritis (EIA). High-resolution peripheral quantitative computed tomography (HR-pQCT) provides superior resolution of bone compared to x-ray, and reliable quantification of joint space [1] and erosions [2]. We used HR-pQCT to quantify changes in joint space, erosion number and size, and bone microarchitecture in EIA patients during the first year of therapy.
Methods: We recruited 47 EIA subjects and performed HR-pQCT (XtremeCT I, Scanco Medical AG, Switzerland) scans of the 2nd and 3rd MCPs of their dominant hand at diagnosis and 1 year later and collected sociodemographic and disease characteristics and disease activity at both timepoints. Erosion number and size were assessed from HR-pQCT images by applying the erosion definition and margin landmarks proposed by SPECTRA [2]. Mean, maximum, and minimum joint space width as well as joint space volume were assessed in 3D [1]. Total bone mineral density (Tt.BMD) was assessed in the distal 12% of the 2nd and 3rd metacarpal heads.
Results: At baseline, 34 met classification criteria for RA [3] and 13 had undifferentiated arthritis. After 1 year several individuals were reclassified: 1 had adult onset StillÕs disease, 1 had Psoriatic Arthritis, and 3 had a self-limited arthritis. The majority received DMARD therapy (89%) and 27% progressed to biologic use. The mean DAS28 improved from 5.4 (SD 1.2) to 2.4 (SD 1.1), and the HAQ decreased from 1.20 (SD 0.72) to 0.41 (SD 0.51). Erosions by HR-pQCT were found in 34% (19) of subjects at baseline, with 32 erosions detected (mean axial width 1.2 (SD 0.7) mm, axial depth 1.8 (SD 1.1) mm, perpendicular width 1.4 (SD 0.9) mm, perpendicular depth 1.8 (SD 1.1) mm. This increased to 40 erosions at 1 year, with 23 subjects remaining free of erosions, 12 having a stable number and 8 having an increased number of erosions. However, only 3 erosions had a depth increase that exceeded the smallest detectable change. At the 3rd MCP, mean and minimum joint space width (mm) decreased by 0.06 (SD 0.11) and 0.082 (SD 0.20), respectively. In contrast there were no significant changes in joint space width or volume at the 2nd MCP joint. There were no significant changes in Tt.BMD in the 2nd or 3rd MC. Type of therapy, CCP, RF, or 1-year remission status did not influence change in Tt.BMD or joint space.
Conclusion: Joint space narrowing progressed and the number of erosions increased despite rheumatologic intervention. HR-pQCT provides greater sensitivity for detection of changes in joint space, erosions and bone microarchitecture.
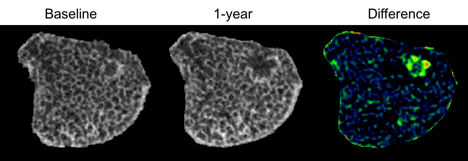
Figure 1. Change in erosion over 1-year follow-up evaluated with HR-pQCT after registration and alignment with baseline image.
References: [1] Barnabe et al, Med Eng Phys, 35: 1540-44, 2013. [2] Barnabe et al, J Rheumatol, 43: 1935-40, 2016. [3] Aletaha et al, Arthitis Rheum, 62: 2569-81, 2010.
To cite this abstract in AMA style:
Manske S, Finzel S, Boyd SK, Barnabe C. Detection of Progression of Radiographic Damage Despite Early and Targeted Therapy in Inflammatory Arthritis Using High-Resolution Peripheral Quantitative Computed Tomography [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/detection-of-progression-of-radiographic-damage-despite-early-and-targeted-therapy-in-inflammatory-arthritis-using-high-resolution-peripheral-quantitative-computed-tomography/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/detection-of-progression-of-radiographic-damage-despite-early-and-targeted-therapy-in-inflammatory-arthritis-using-high-resolution-peripheral-quantitative-computed-tomography/