Session Information
Date: Sunday, November 13, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster II: Manifestations
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Poor sleep quality is a common complaint of patients with SLE. Although chronic sleep disruption is known to drive circadian rhythm disorders, the effects of poor sleep quality have not yet been elucidated in SLE. Actigraphy is a validated approach to objectively assess 21 sleep variables and motor activity using a noninvasive accelerometer. In addition, actigraphy can characterize circadian dysfunction by assessments of activity. We examine the relationship of actigraphy data from SLE patients with 1) disease activity and 2) subjective patient-reported outcome measures of sleep quality.
Methods: 76 consented subjects from the Washington University Lupus Clinic with classified SLE were enrolled from May 2015-2017. Participants wore a wrist-mounted actigraph (Micro Motionlogger, Ambulatory Monitoring Inc, Ardsley, NY) for one week. Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), Patient Reported Outcomes Measurement Instrument System (PROMIS)-Sleep Related Impairment (SRI), and PROMIS-Sleep Disturbance (SD) survey instruments were administered to measure subjective sleep quality. SLEDAI-2000 Responder Index-50 (S2K RI-50) assessed disease activity ( >4, active SLE). Actigraphy data were analyzed using Action W (Ambulatory Monitoring Inc), and circadian variables were derived using ClockLab (Actimetrics, Wilmette, IL). Unpaired Student t tests (two-sided, α < 0.05) were used to compare sleep quality and circadian dysfunction in patients with active versus inactive disease. Pearson correlation coefficient was used to assess correlation of actigraphy and circadian variables with subjective sleep quality. Statistical analyses were performed using SPSS Statistics (IBM, Armonk, NY).
Results: Average patient age was 40.5 years, 93.4% were female, 33.0% were employed full time, and 34.7% were on glucocorticoids.
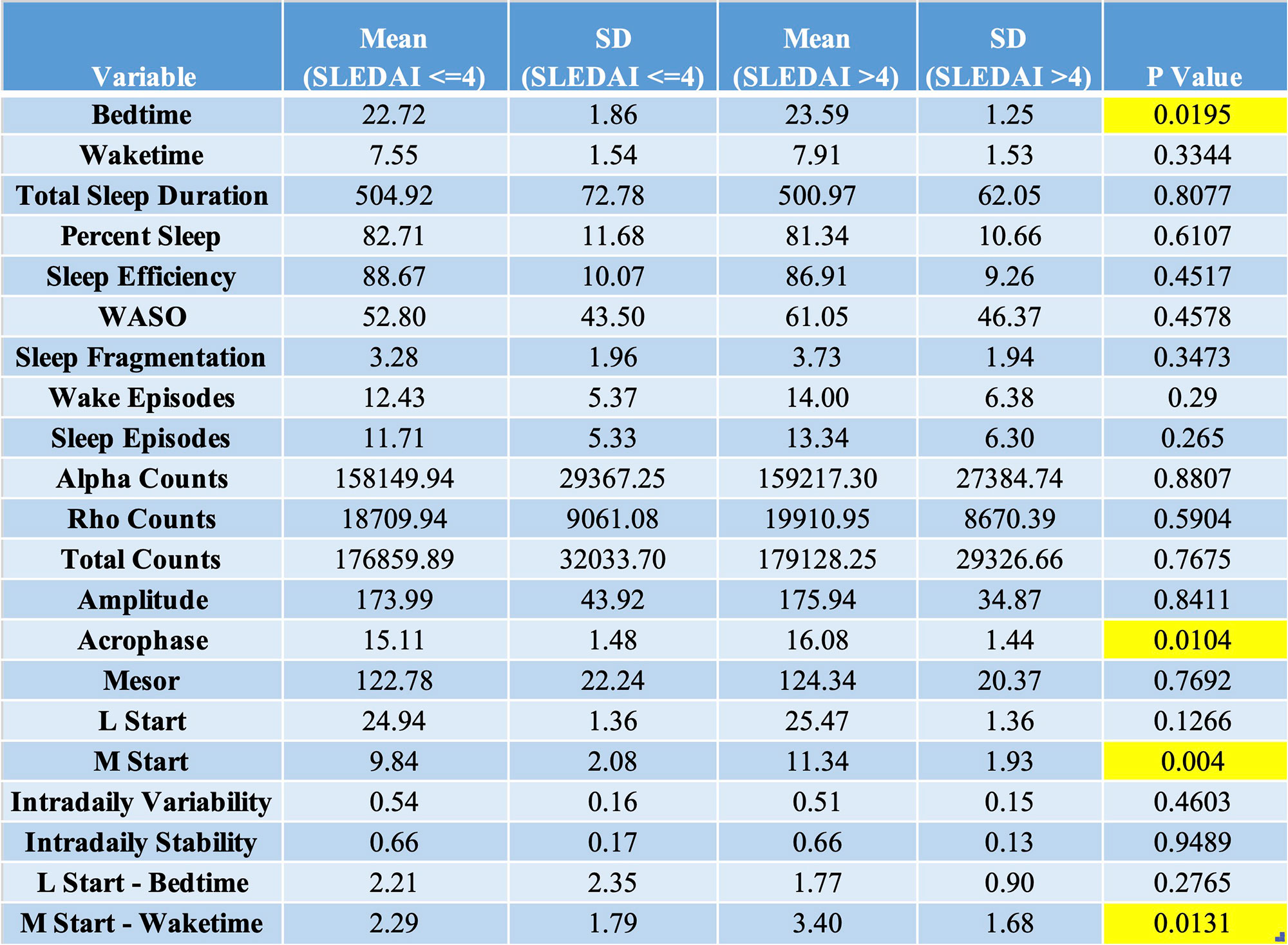
No differences in actigraphic measures of sleep quality (e.g., total sleep duration, percent sleep, wake after sleep onset, etc.) were observed in active versus inactive disease. Active SLE was associated with phase-dependent circadian variables including bedtime (p=0.02), acrophase (p=0.01, peak of circadian activity), M start (p=0.004, beginning of most active hours), and M start – waketime (p=0.01, discrepancy between natural circadian rhythm and actual activity pattern) (Table 1).
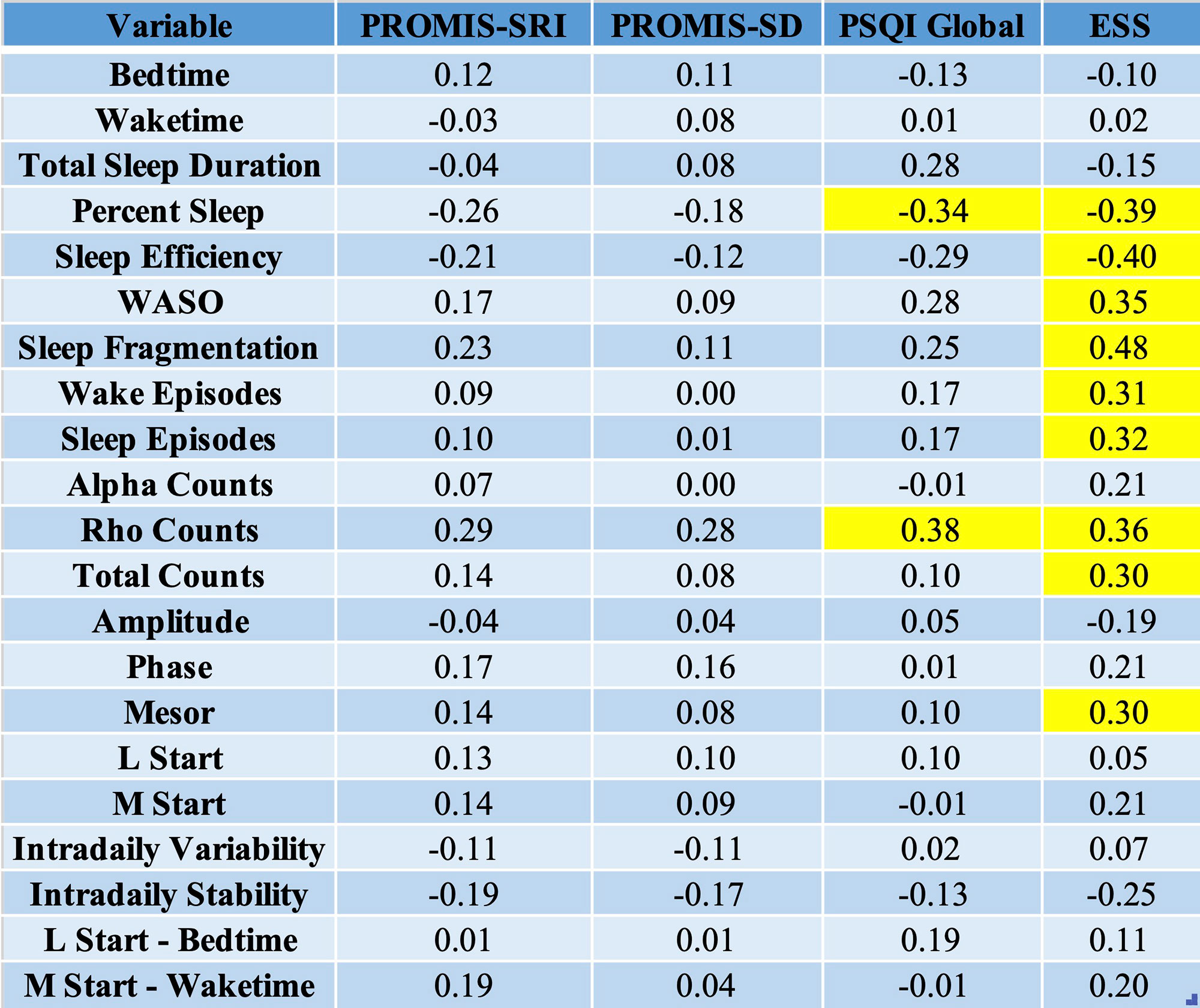
PROMIS-SRI and PROMIS-SD showed no correlation with actigraphy or circadian measures, while PSQI and ESS correlated moderately with % sleep and rho counts (activity during sleep period), and ESS additionally showed modest correlation with measures such as sleep efficiency, sleep and wake episodes, and MESOR (measure of mean activity level) (Table 2).
Conclusion: Changes in circadian phase, but not sleep quality, is associated with SLE disease activity, with a phase delay in those with active disease. The ESS was the PRO that most highly associated with several actigraphy-assessed sleep parameters, including sleep efficiency and fragmentation. Circadian dysfunction may be an underlying cause for other widely experienced symptoms of SLE including cognitive dysfunction and fatigue. Future work will focus on examining this relationship.
To cite this abstract in AMA style:
Stankey C, Chu P, Hinze A, McMorrow L, El-Qunni A, Sen D, Eisen S, Ju Y, Kim A. Delayed Sleep Phase Syndrome Characterizes Circadian Disorder in Patients with Active SLE [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/delayed-sleep-phase-syndrome-characterizes-circadian-disorder-in-patients-with-active-sle/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/delayed-sleep-phase-syndrome-characterizes-circadian-disorder-in-patients-with-active-sle/