Session Information
Date: Monday, November 18, 2024
Title: Abstracts: SpA Including PsA – Diagnosis, Manifestations, & Outcomes II
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Clinical enthesitis occurs in 30-40% of psoriatic arthritis (PsA) patients, but its clinical diagnosis is challenging due to similarities to non-specific entheseal pain. Despite OMERACT’s standardization of ultrasound (US) entheseal lesions, a unified definition for inflammatory enthesitis remains vague. This study aims to develop data- and expert-driven diagnostic criteria to differentiate inflammatory enthesitis at the single enthesis level from non-specific sonographic enthesopathy.
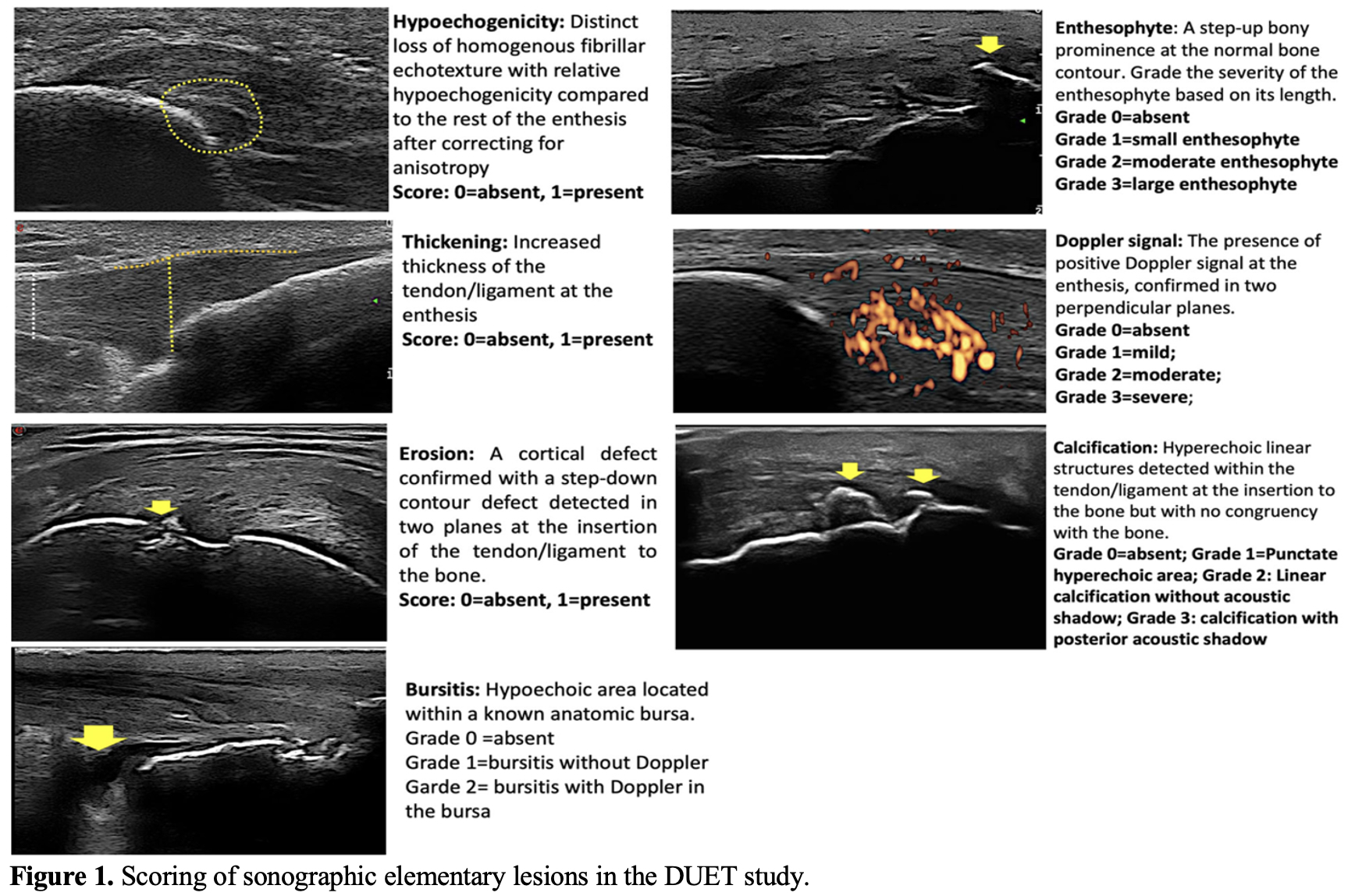
Methods: An expert panel of 10 sonographers who participated in the Diagnostic Ultrasound Enthesitis Tool (DUET) study reviewed 90 US scans (stored as video clips) of PsA patients. These represented various severities of entheseal lesions from 6 different sites. Each investigator rated each scan on a scale from -10 (definite “No”) to +10 (definite “Yes”) for the likelihood of representing enthesitis. To be considered “Definite enthesitis” ≥ 70% of readers had to rate it with ≥ 70% certainty (+7 or higher). Sonographers also noted the sonographic features influencing their ratings. Consensus scoring (3 central readers) of elementary lesions was taken from the DUET study (Figure 1)1. Descriptive statistics and Chi-square tests were used to report differences in elementary lesions across categories.
Results: Preliminary results show that 29 (32.2%) scans were classified as “Definite enthesitis”, 21 (23.3%) as “Definite not enthesitis”, and 40 (44.5%) had no consensus (“Uncertain”).
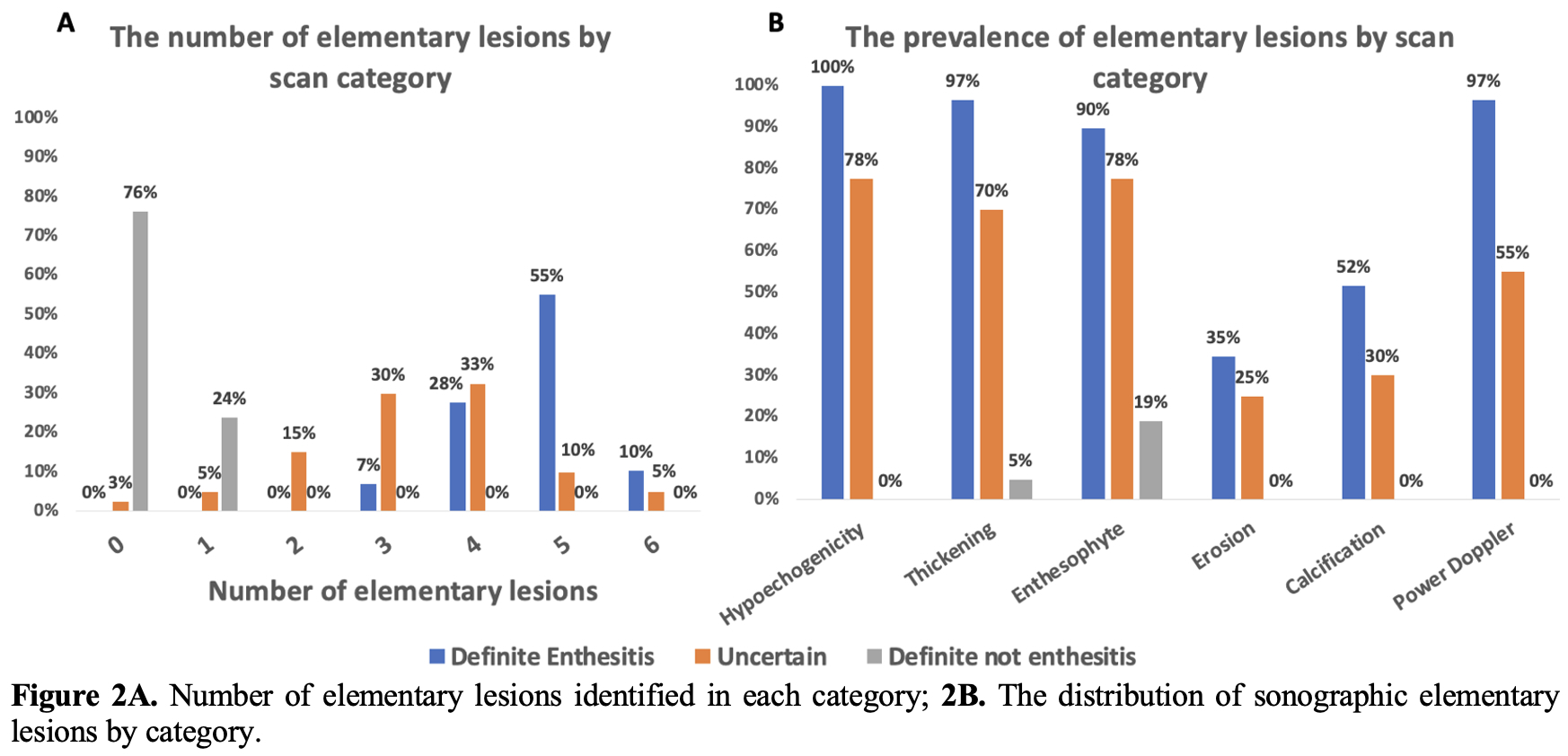
“Definite enthesitis” scans had more elementary lesions compared to “Uncertain” and “Not enthesitis” scans (Figure 2A-B). 93.1% of “Definite enthesitis” scans had a combination of ≥ 4 elementary lesions, while “Uncertain” and “Not enthesitis” scans mostly had 3 or fewer lesions (52.5% and 100%, respectively).
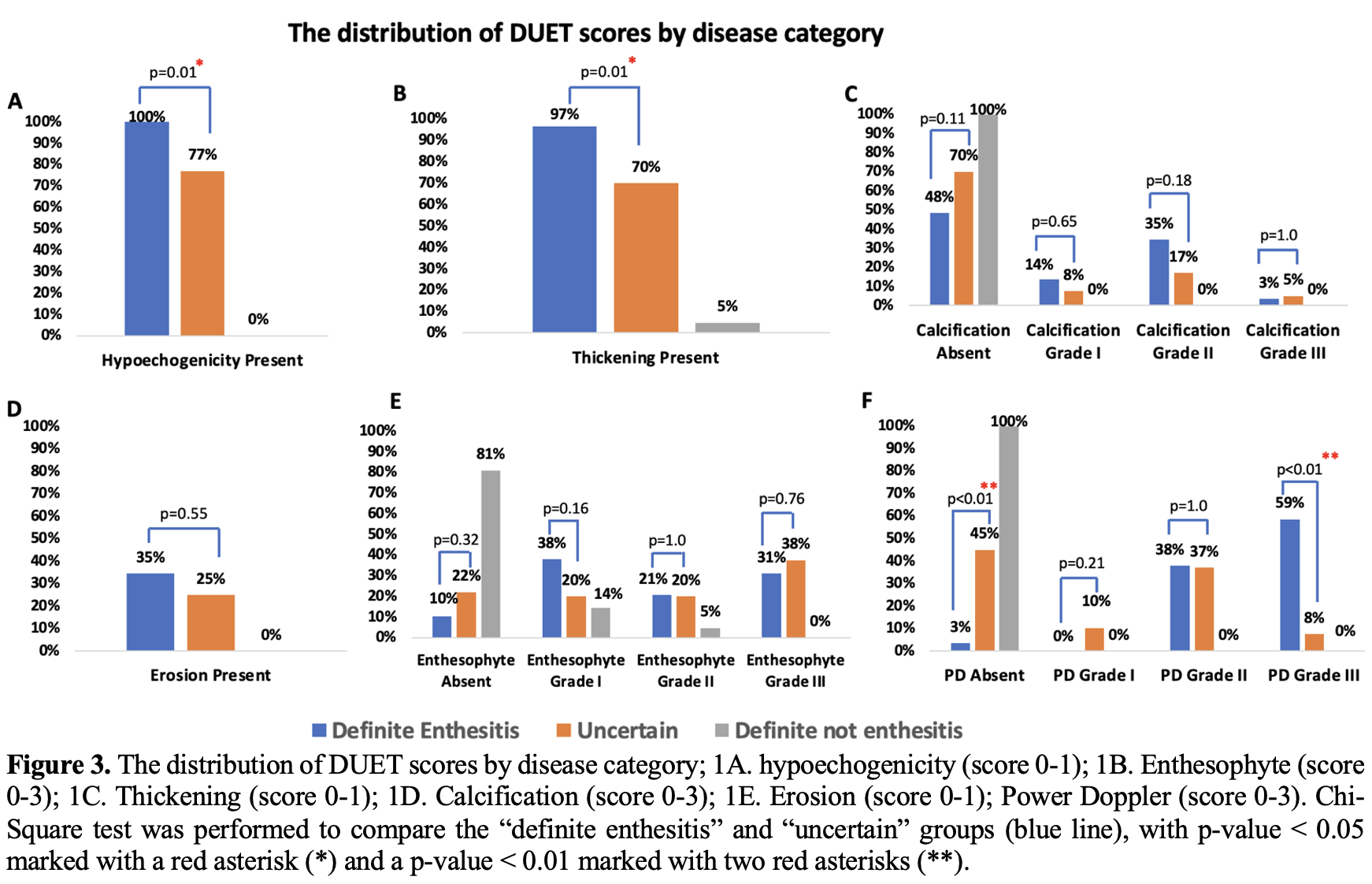
The DUET scoring of elementary lesions and Chi-Square significant differences are shown in Figure 3A-F, highlighting the differences of Hypoechogenicity, Thickening, and Power Doppler (PD) between “Definite enthesitis” and “Uncertain” groups. Most “Definite enthesitis” scans had PD ≥ 2 (n=28, 96.5%), with the remaining scan showing significant B mode abnormalities, including erosions. The “Not enthesitis” group mostly had no elementary lesions (76.2%), with only 4 scans showing isolated enthesophytes and 1 with thickening. “Uncertain” scans showed a mixed combination of elementary lesions, with 55% having positive PD. Unlike the OMERACT definition of PD location in enthesitis, 68.1% of the PD was ≥ 2 mm from the insertion site, which was an important factor for classifying them as “Uncertain”.
Conclusion: The presence of inflammatory elementary lesions drives the opinion towards a categorization of definite enthesitis, particularly when high grade PD signal is present and when four or more elementary lesions are combined. Isolated enthesophytes, common in the general population, do not indicate inflammatory enthesitis. These initial insights will form the basis for an inflammatory enthesitis definition.
Reference
- Eder L, Aydin S, Kaeley G. The Reliability of Scoring Sonographic Entheseal Abnormalities – the Diagnostic Ultrasound Enthesitis Tool (DUET) Study [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10).
To cite this abstract in AMA style:
Lucas Ribeiro A, Aydin S, Kaeley G, Afgani F, Bakewell C, Rosemffet M, Kohler M, Haddad A, Stoenoiu M, Polachek A, marin j, Katz A, Eder L. Defining Sonographic Enthesitis in Psoriatic Arthritis: Developing a Data- and Expert-driven Diagnostic Criteria for Inflammatory Enthesitis at the Single Enthesis Level [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/defining-sonographic-enthesitis-in-psoriatic-arthritis-developing-a-data-and-expert-driven-diagnostic-criteria-for-inflammatory-enthesitis-at-the-single-enthesis-level/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/defining-sonographic-enthesitis-in-psoriatic-arthritis-developing-a-data-and-expert-driven-diagnostic-criteria-for-inflammatory-enthesitis-at-the-single-enthesis-level/