Session Information
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Several reports indicate that patient global assessment (PATGL) may elevate DAS28 (disease activity score 28) and/or other indices in patients with rheumatoid arthritis (RA), who might otherwise meet criteria for remission, leading to suggestions to consider deletion of PATGL from RA remission criteria. However, RA patients who are classified as in remission by DAS28 may have elevations of other DAS28 components, swollen joint count (SJC), tender joint count (TJC), erythrocyte sedimentation rate (ESR), or C-reactive protein (CRP). A meta-analysis indicated that DAS28 was significantly higher in patients with RA who had comorbid fibromyalgia (FM+) vs FM- patients, and that both TJC and PATGL were higher in FM+ vs FM- RA groups. We analyzed in detail the four DAS28 components to explain elevated DAS28 in FM+ vs FM- RA patients
Methods: We collected articles from the meta-analysis report and conducted a further PubMed search according to “rheumatoid arthritis and fibromyalgia and disease activity” to identify reports which presented details of mean or median levels of DAS28 and each of the 4 components, TJC, SJC, ESR or CRP, and PATGL in FM+ vs FM – RA groups. We compiled mean or median DAS-28 ESR (no reports with DAS28-CRP met inclusion criteria), and the four DAS28 components in FM+ vs FM- patients, TJC and SJC as 0-28 joint counts, ESR as mm/hr, and PATGL as 0-100. Ratios of FM+/FM- patients were calculated. The medians were calculated of reported means or medians for DAS-28 and its 4 components in the FM+ and FM- RA groups, and of ratios of FM+/FM- groups.
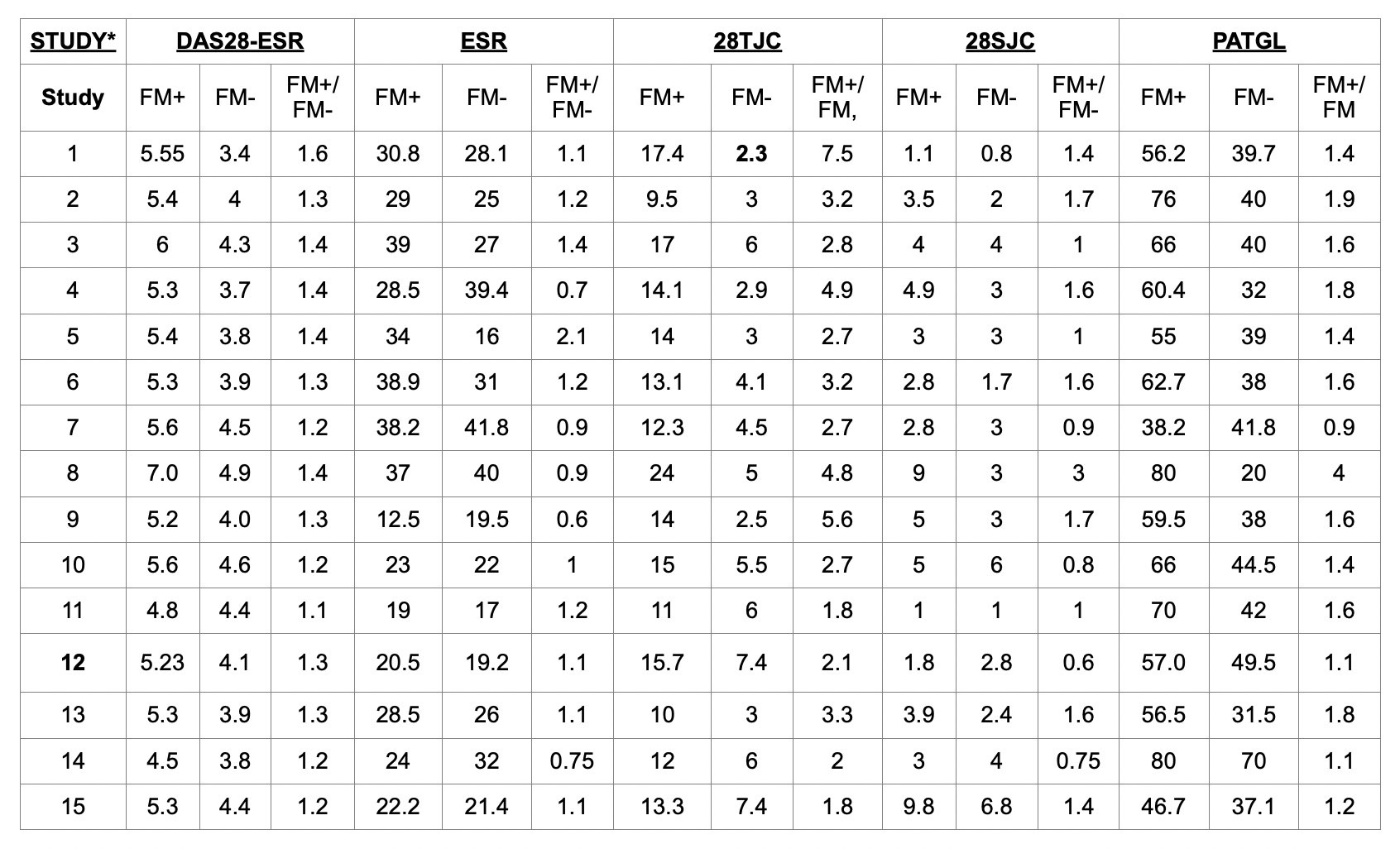
Results: 15 studies were included, 10 from the previous meta-analysis and 5 from the PubMed search; 12 presented DAS-28 as means and standard deviations and 3 as medians and confidence intervals. Median of mean or median DAS28 in FM+ vs FM- groups was 5.3 (range 4.5-7.0) vs 4 (range 3.4-4.9) (Table 1). Median of mean or median ESR in FM+ vs FM- groups was 28.5(range 12.5-39) vs 26 (range 16-41.8). Median of means or median of TJC in FM+ vs FM – groups was 14 (range 9.5-24) vs 4.5 (range 2.3-7.4). Median of mean or median SJC in the FM+ vs FM – groups was 3.5 (range 1-9.8) vs 3 (range 0.8-6.8). Median of means or medians PATGL in RA FM+ vs FM- groups was 60.4 (range 38.2-80) vs 39.7 (range 20-70). Both TJC and PATGL were higher in each of the 15 studies in FM+ vs FM- RA patients. The median ratio of DAS-28 ESR in FM+ vs FM- groups was 1.4 (range 1.1-1.6). Median ratios of DAS28 components in FM+/FM- groups were 3.2 for TJC, 1.6 for PATGL, 1.4 for SJC, and 1.1 for ESR
Conclusion: The data confirm and extend findings from the meta-analysis that DAS28 is elevated significantly in FM+ vs FM- RA patients. The median ratio of FM+ vs FM- groups for TJC was 3.2, double that of PATGL. Therefore, removal of PATGL from DAS28 for patient assessment and/or for criteria for remission would leave substantial elevations in FM+ RA patients resulting from elevated TJC. This information may be relevant to possible revision of RA remission criteria, as well as to monitoring of RA patients in clinical trials, other clinical research, and routine rheumatology care
To cite this abstract in AMA style:
Kannayiram S, Schmukler J, Goodson N, Pincus T. DAS28 (disease Activity Score) Elevations in Patients with Rheumatoid Arthritis (RA) Who Have Comorbid Fibromyalgia Are Explained by Elevated Tender Joint Counts as Much as by Elevated Patient Global Assessment [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/das28-disease-activity-score-elevations-in-patients-with-rheumatoid-arthritis-ra-who-have-comorbid-fibromyalgia-are-explained-by-elevated-tender-joint-counts-as-much-as-by-elevated-patient-global/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/das28-disease-activity-score-elevations-in-patients-with-rheumatoid-arthritis-ra-who-have-comorbid-fibromyalgia-are-explained-by-elevated-tender-joint-counts-as-much-as-by-elevated-patient-global/