Session Information
Date: Tuesday, November 12, 2019
Title: Systemic Sclerosis & Related Disorders – Clinical Poster III
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Pulmonary arterial hypertension (PAH) is a life-threatening complication of systemic sclerosis (SSc), thought to be more commonly found among the limited cutaneous (lcSSc) compared to diffuse (dcSSc) disease subtype. Since lcSSc is associated with better prognosis, it is unclear whether a higher occurrence of PAH in lcSSc is a reflection of survival bias, especially when longer disease duration and older age increase the risk of PAH. We assessed survival and incidence of PAH, after accounting for death as competing event, in a large multi-center cohort of SSc patients, and explored predictors of PAH development and survival.
Methods: The study consisted of 1689 SSc patients from Canadian Scleroderma Research Group registry, followed for up to 14 years. To compare cumulative incidence between disease subsets, a competing risk analysis (Fine-Gray model with death as competing event) unadjusted and adjusted for sex, age and SSc-related autoantibodies was performed (SAS 9.4). Survival was analyzed by Kaplan-Meier with Log-Rank (Mantel Cox) test; Cox proportional hazards analysis with demographic, clinical, and laboratory characteristics as predictor variables was used to develop prediction models for PH (SPSS 25.0).
Results: Out of 1431 patients (43% dcSSc, 57% lcSSc, mean age at SSc diagnosis 48±13, follow up 3.5±2.9 yrs., range 1-14 yrs.) with sufficient data for PAH, 157 patients had PAH either confirmed by RHC or post mortem. Regardless of SSc subtype, patients with PAH had more severe disease (by HAQ-DI and patient’s global assessment of health) and higher mortality (74% vs 11%, p< 0.0001), compared to those without PAH (Table 1). The lcSSc patients with PAH were older at SSc diagnosis and had a longer disease duration from Raynaud’s phenomenon (RP), compared to lcSSc without PAH. The dcSSc patients with PAH had more severe peripheral vascular (SHAQ RP and finger ulcers) and gastrointestinal (SHAQ intestinal problems) vs dcSSc without PAH. 47% of patients with PAH died: 45 lcSSc and 29 dcSSc. Male gender and anti-Scl70 were associated with earlier development of PAH from both SSc diagnosis (p< 0.0001 and p=0.002, respectively) and first non-RP symptom (p< 0.0001 and p=0.001, respectively).To avoid left-censoring problem, 113 pts with PAH diagnosed at or before baseline registry visit were excluded from the cumulative incidence and survival analyses. Cumulative incidence of PAH from the onset of first non-RP symptom was higher in dcSSc than in lcSSc after accounting for death as competing event in unadjusted, but not adjusted competing risk analysis (see Table 2 and Figure). Survival (mean±SE) from PAH onset was similar in lcSSc and dcSSc (44±8 mo vs 38±7 mo, p=0.59).
Conclusion: Cumulative incidence of PAH from the onset of first non-Raynaud’s phenomenon symptom was not higher in lcSSc, after accounting for death as competing event and adjusting for age, sex and antibody status. Males and a-Scl-70-positive patients developed PAH earlier
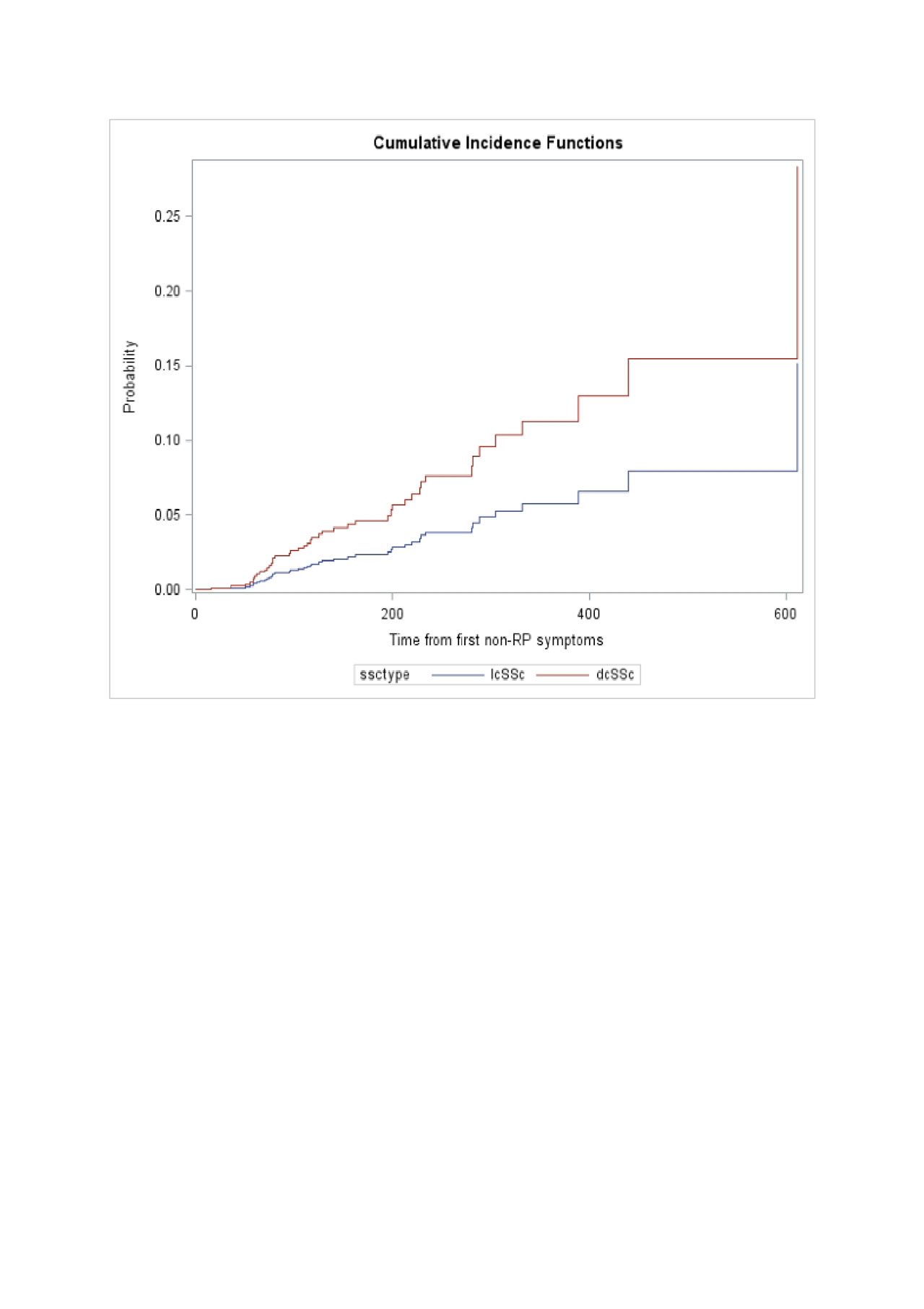
Image for abstract
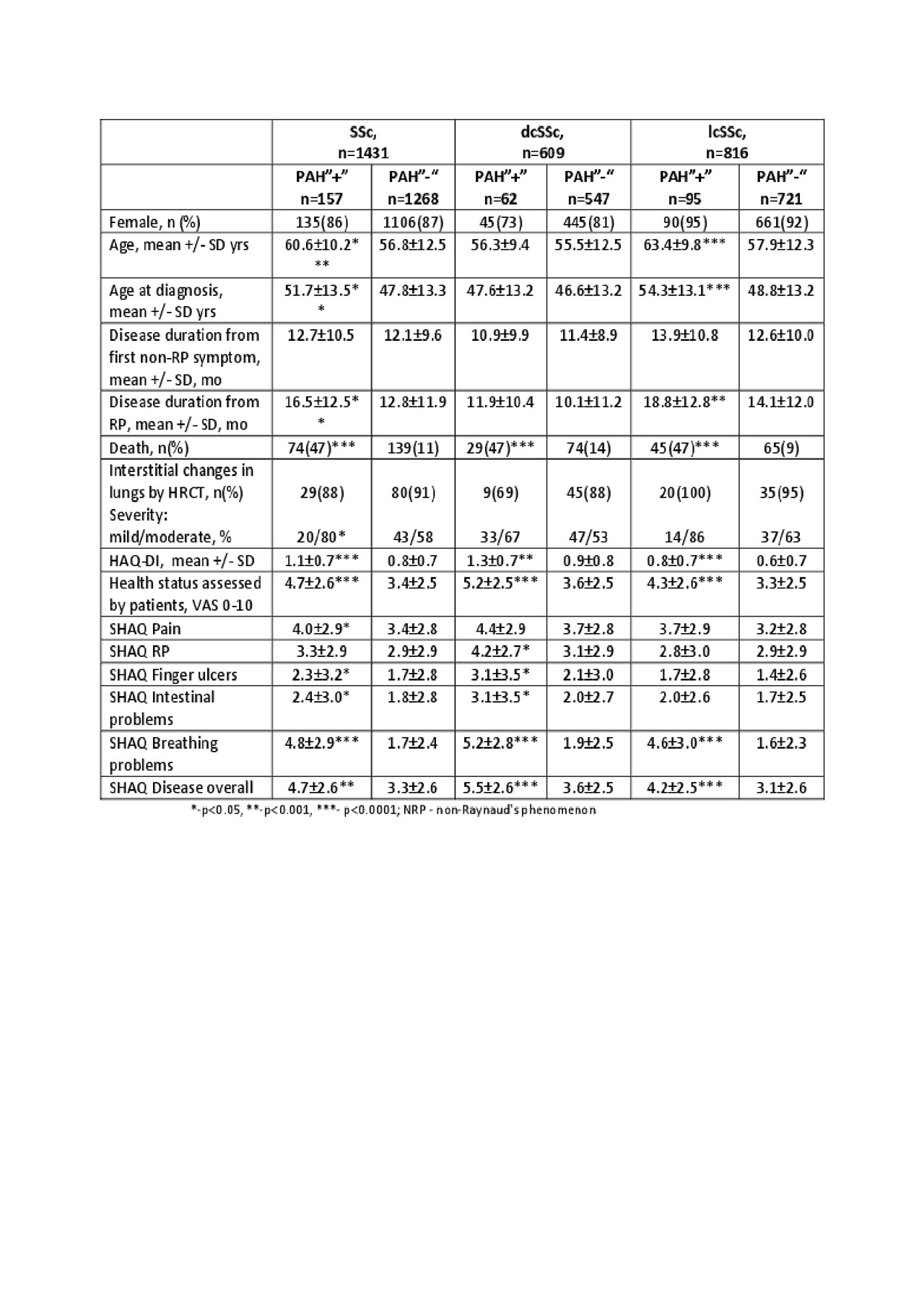
Table 1 for abstract
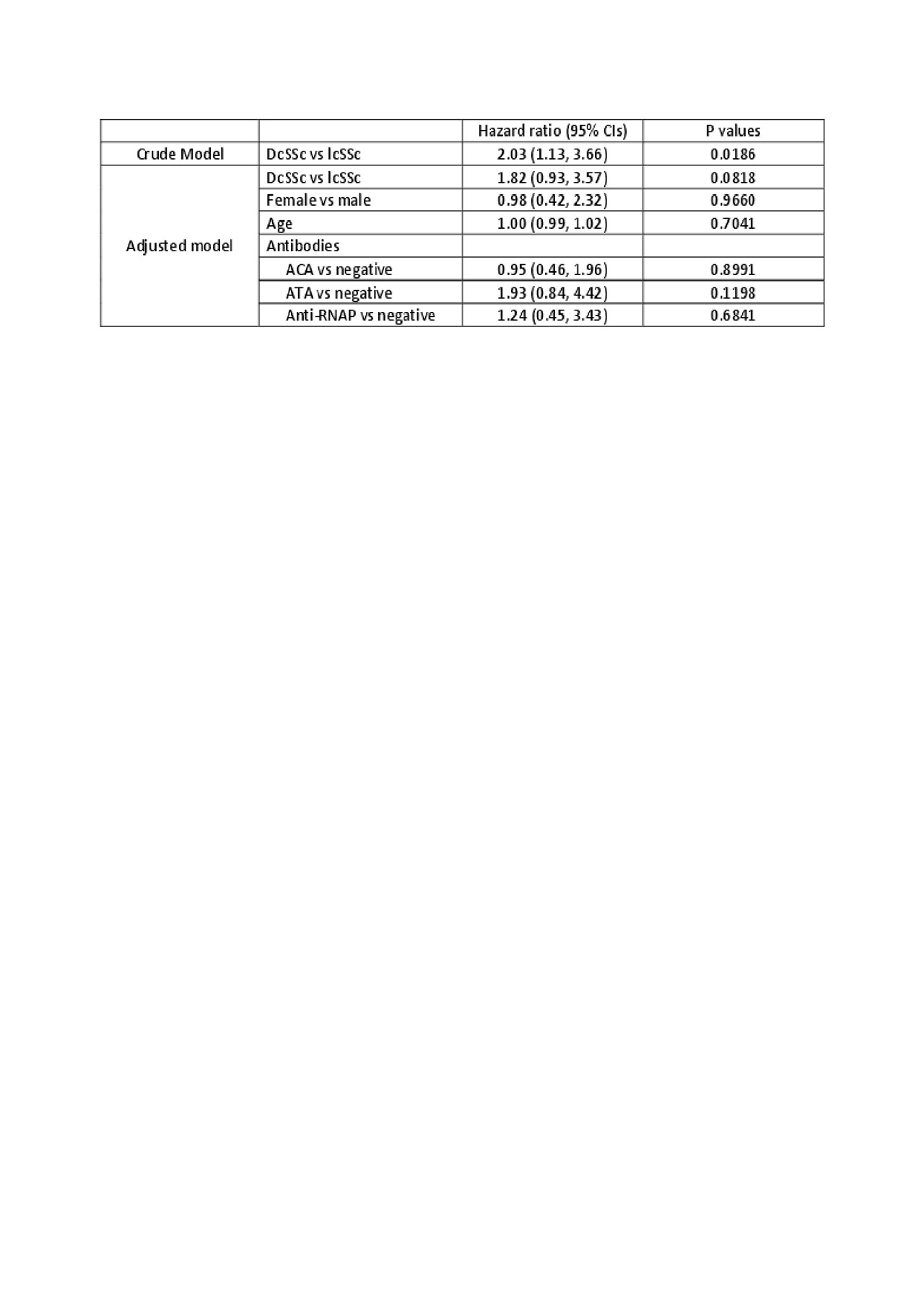
Table 2 for abstract
To cite this abstract in AMA style:
Nevskaya T, Jiang Y, Wang M, Pope J. Cumulative Incidence, Survival and Predictors of Pulmonary Arterial Hypertension in Disease Subsets of Systemic Sclerosis: PAH Is Not Increased in Limited vs Diffuse Patients by Adjusted Competing Risk Analysis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/cumulative-incidence-survival-and-predictors-of-pulmonary-arterial-hypertension-in-disease-subsets-of-systemic-sclerosis-pah-is-not-increased-in-limited-vs-diffuse-patients-by-adjusted-competing-ris/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cumulative-incidence-survival-and-predictors-of-pulmonary-arterial-hypertension-in-disease-subsets-of-systemic-sclerosis-pah-is-not-increased-in-limited-vs-diffuse-patients-by-adjusted-competing-ris/