Session Information
Date: Sunday, November 5, 2017
Title: Rheumatoid Arthritis – Clinical Aspects I: Cardiac Comorbidities
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose:
Patients with DM have increased coronary microvascular dysfunction (CMD) compared to the general population, leading to higher rates of cardiac death despite normal perfusion scans. While CMD is also thought to play a role in excess cardiovascular (CV) risk in RA, studies are limited. CMD can be detected using coronary flow reserve (CFR), calculated using data from clinically available stress myocardial perfusion PET scans. A pathognomonic sign of CMD is a patient with normal perfusion on a stress test, but impaired CFR. The objective of this study was to compare the frequency of CMD in RA compared to DM among subjects with normal perfusion scans.
Methods:
We performed a retrospective study within a tertiary care hospital registry of patients who received stress myocardial perfusion PET scans as part of routine clinical care between 1/1/2006-1/1/2016. The registry contains data on demographics, CV risk factors, stress test results (normal vs abnormal perfusion), CFR, and adjudicated mortality outcomes. RA patients were identified using a validated algorithm and their medical records were reviewed to confirm prevalent RA at the time of the stress test. We created a DM comparison group, matching to RA by age, gender, race, and year of stress test. Among patients with normal perfusion scans, we compared the distribution of CFR in RA compared to DM, and their mean CFRs using the student’s t-test. We performed chi-square tests to determine whether an impaired CFR (CFR<2) was associated with a higher proportion of all-cause mortality in the RA and DM groups.
Results:
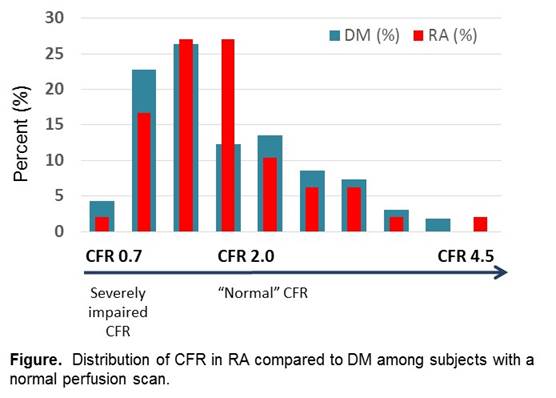
We studied 49 RA and 163 DM patients with normal perfusion scans. The RA patients had a mean age of 64.4 years at the time of their scan, 59.2% white, 51% seropositive. There was no significant difference between the age, gender, hypertension, dyslipidemia, family history of CVD, or smoking status between the RA and DM groups. The mean CFR was 2.02 for RA and DM, with a similar distribution of CFR between the two groups (p=0.98) (Figure). During a median follow-up of 5.4 years, DM with impaired CFR had a significantly higher all-cause mortality than those with normal CFR (p=0.02); a similar trend was observed in RA (p=0.29) (Table).
Conclusion:
In patients undergoing clinically indicated stress tests with normal perfusion scans, we observed a similar distribution of CMD in RA compared to DM. These data suggest that CMD may contribute to the excess CV risk in RA as in DM. CFR, calculated from clinically available stress myocardial perfusion PET scans is a promising imaging biomarker to guide CV risk assessment in RA.

To cite this abstract in AMA style:
Liao KP, Cremone G, Lam E, Yu Z, Hainer JM, Morgan V, Bibbo C, Di Carli M. Coronary Microvascular Dysfunction in Rheumatoid Arthritis Compared to Diabetes Mellitus in Patients without Obstructive Coronary Artery Disease [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/coronary-microvascular-dysfunction-in-rheumatoid-arthritis-compared-to-diabetes-mellitus-in-patients-without-obstructive-coronary-artery-disease/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/coronary-microvascular-dysfunction-in-rheumatoid-arthritis-compared-to-diabetes-mellitus-in-patients-without-obstructive-coronary-artery-disease/