Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: To estimate the prevalence of subjects with osteoarthritis (OA) having led to doctor consultation.
Methods: The Skåne Health Care Register (SHCR) is a legislative, mandatory register based on physicians’ International Classification of Diseases (ICD) 10 diagnostic codes. The register covers all in- and outpatient health care in southern Sweden (total population 1.3 million). We identified all adult (20 years of age or older) patients having received the diagnosis of knee OA (ICD-10: M17), hip OA (M16), hand OA (M15.1, M15.2, M18, M19.0D, M19.1D or M19.2D), spine OA (M47) and OA in other locations, i.e., elbow, foot, shoulder, or other joints (M19 different from M19.0D, M19.1D and M19.2D) or polyarthrosis (M15 different from M15.1 and M15.2) during the years 1999 until 2011. We obtained point estimates of consultation prevalence by Dec 31st 2011 by cross referencing with the population register to exclude subjects who had relocated from the county or were deceased. To obtain valid prevalence estimates and confidence intervals in presence of missing data on ICD-10 codes (mainly in private care and in primary care before the year 2004), we used the multiple imputation technique. The variables included in the imputation model were age, sex and clinic and their interactions, year, if consulted physiotherapist, if consulted psychiatrist, residential area, civil status, indicator for in- or outpatient care and the person as a random effect to account for the correlation between visits made by the same patient.
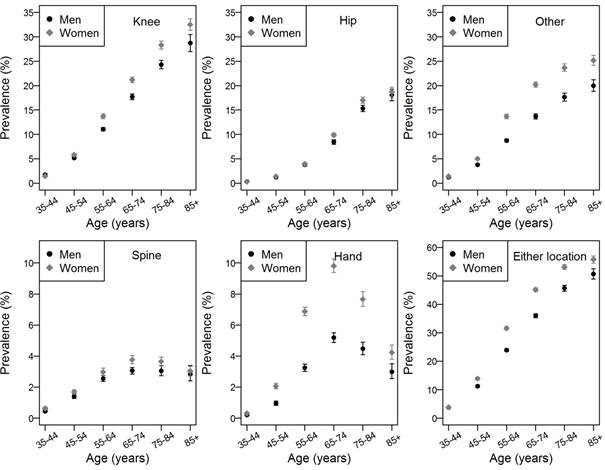
Results: The adult consultation prevalence of OA (any location) was 18.6% (95%CI: 18.4%; 18.7%), 15.8% (95%CI: 15.6%; 16.0%) for men and 21.3% (95%CI: 21.0%; 21.5%) for women. The most common location was knee OA with a prevalence of 9.0%, followed by OA of other joints –7.5%, OA of the hip –4.0%, hand OA – 2.7% and spine OA with the consultation prevalence of 1.6%. The consultation prevalence in population aged 65 or more was 45.5%, 40.5% for men and 49.6% for women. If we considered a diagnosis of joint pain (ICD-10: M25.5) and age 45 or older as OA, the consultation prevalence of OA in extremities increased from 29.6% to 38.5%. The age and sex-specific patterns are displayed in the graph (Figure).
Of subjects who consulted for OA 28% had OA diagnosed in more than one location, knee OA and other OA being the most common combination (12.5%).
Conclusion: The high doctor consultation prevalence of OA in extremities, 18.6% of all adults, 45.5% of all above 65 years of age, shed light on the burden on the health care system and warrants concerns with a steadily ageing and increasingly obese population. It reinforces the need for improved OA patient care and preventive strategies as well as an increased need for join replacement operations.
Figure. The prevalence of osteoarthritis by location, sex and age. Vertical bars represent the 95% confidence intervals.
Disclosure:
A. Turkiewicz,
None;
I. F. Petersson,
None;
J. Björk,
None;
L. E. Dahlberg,
None;
M. Englund,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/consultation-prevalence-of-osteoarthritis-in-southern-sweden/