Session Information
Date: Sunday, November 8, 2015
Title: Osteoarthritis - Clinical Aspects Poster I: Treatments and Metabolic Risk Factors
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose:
The Outcome Measures in Rheumatology (OMERACT) working group
on hand osteoarthritis (OA) has endorsed a preliminary set of core domains for
outcome measures in clinical trials. One domain is joint activity, reflecting
the underlying osteoarthritic process, such as inflammation and/or subchondral
bone activity, leading to pain and destruction.
The Doyle Index (DI), a measurement of joint tenderness, is
proposed as an instrument to assess joint activity, however validity and its
added value over other domains like self-reported pain is unknown. Therefore, construct
validity of the DI is investigated.
Methods:
Data
were used of two cohorts with primary hand OA patients: HOSTAS (n=507, mean (SD) age 61 (9) years,
86% women) and ECHO (n=56, age 62 (9) years,
86% women). Self-reported pain was assessed by
Australian/Canadian Hand OA Index
(AUSCAN, Likert scale, 0-20) and Visual Analogue Scale (VAS) 1-100. Tenderness
on palpation (0-3) was assessed in24 joint units: all DIP, PIP, 1st IP,
1st MCP and 1st CMC joints individually and 2nd-5th
MCP joints as one joint group. In each patient the DI was the summated score
of the 24 joint units (max. 72).
Contrast-enhanced MRI of the right DIP and PIP joints (8
joint units) were performed in a subgroup of HOSTAS (n=93) and images were
scored for synovitis and bone marrow lesions (BMLs), both 0-3, following
standardized methods. Ultrasound (US) was performed in the ECHO study and all hand
joints (the same 24 joint units as in DI) were scored for grey scale (GS)
synovitis and power Doppler signal (PDS), both 0-3, following standardized
methods.
MRI or US scores were summated scores of synovitis and BMLs
or GS synovitis and PDS, respectively, of all imaged joint units.
To assess construct
validity, first, non-parametric correlation coefficients between DI and self-reported
pain or US or MRI scores were calculated. Subsequently, quartiles of DI (lowest
vs highest) of MRI and US scores were compared with Mann-Whitney U test.
Results:
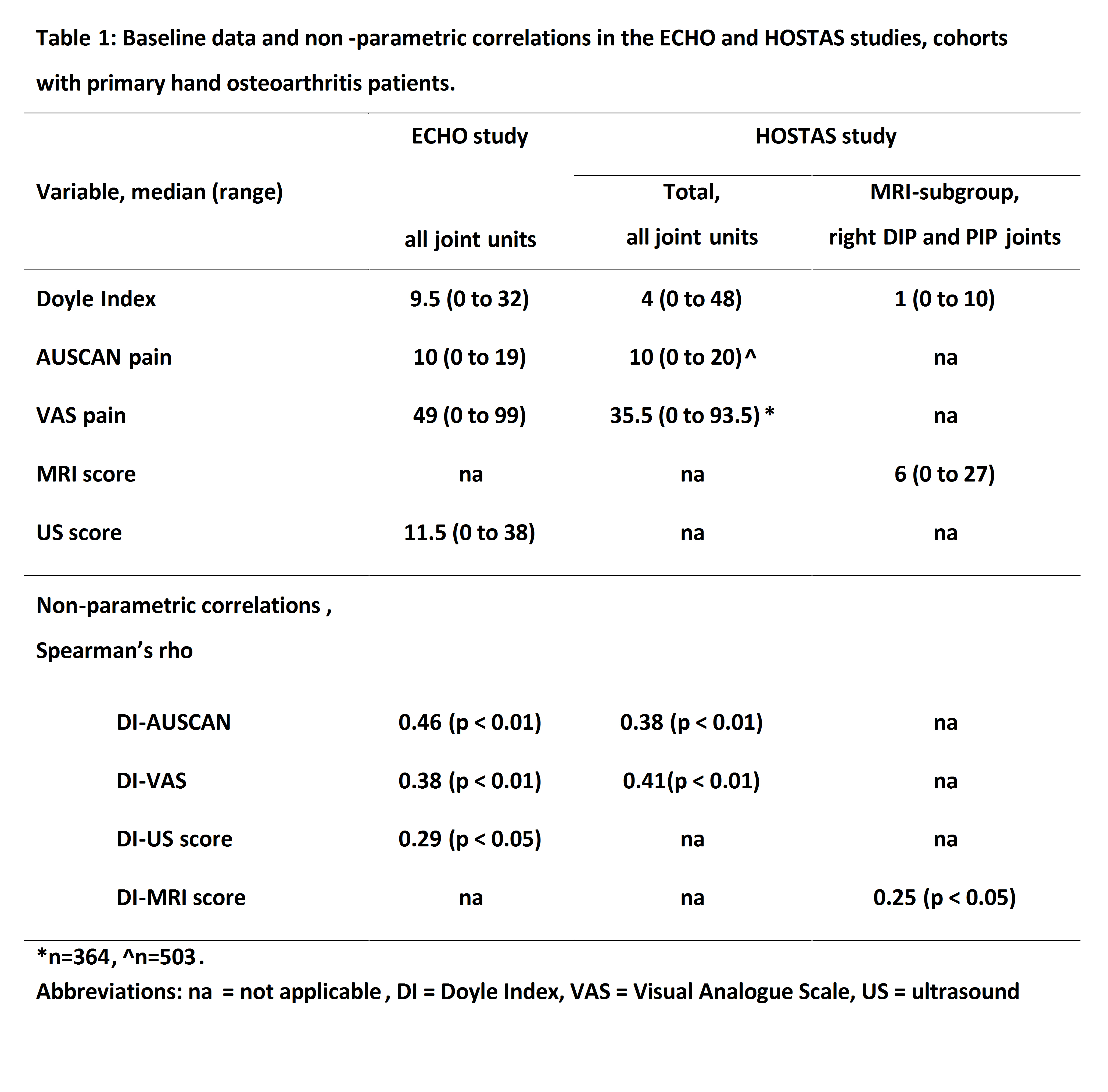
Baseline data and non-parametric correlations are depicted
in table 1. DI varied from 0 to 48 and correlated moderately to self-reported
pain in both studies.
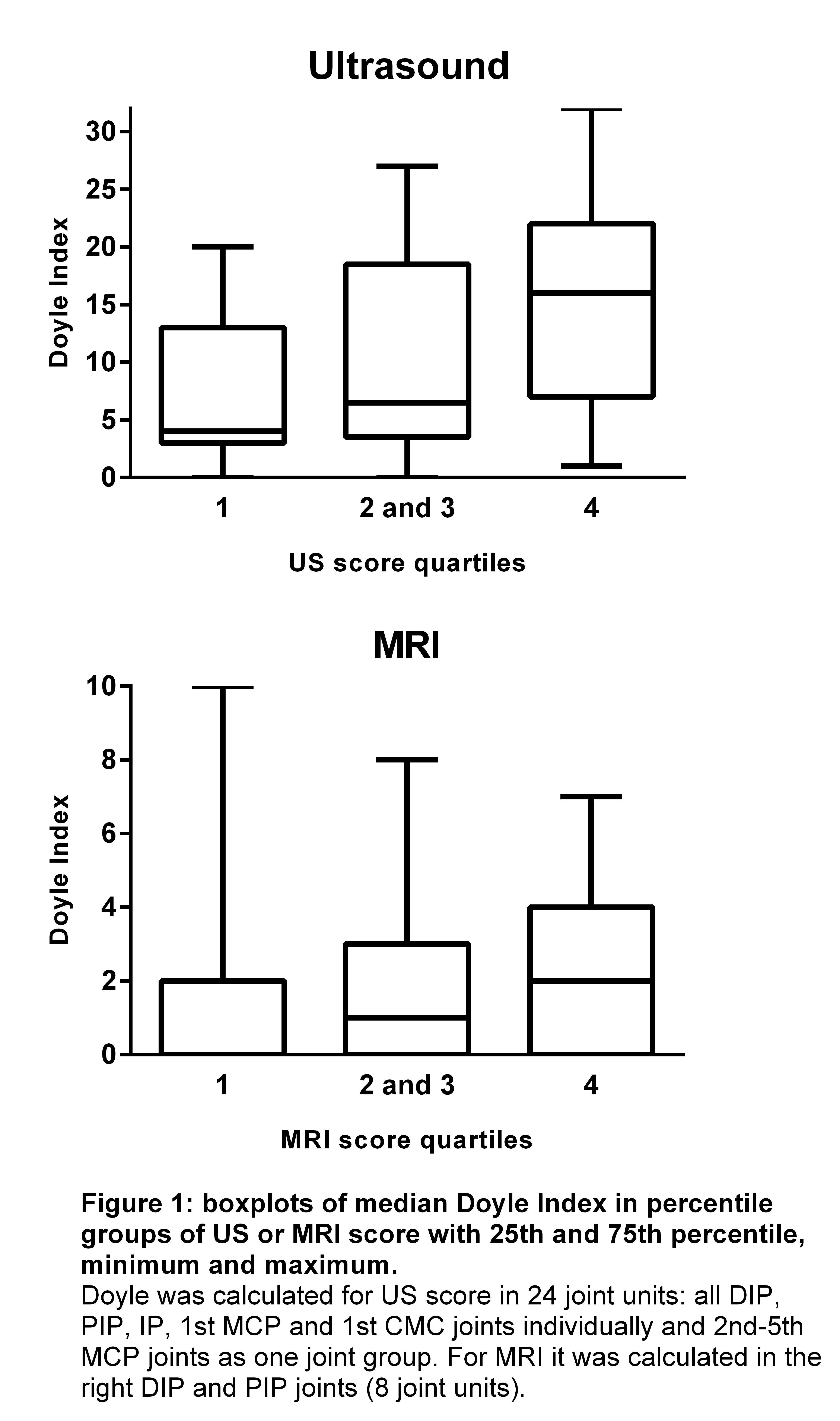
Correlations for DI and US and MRI scores were low. Median
DI differed between lowest quartile and highest quartile scores (figure 1) for the
US score (p=0.050) and MRI score (p=0.066).
Conclusion:
Doyle Index seems a promising instrument to assess joint
activity in clinical trials in hand OA. Further work on metric properties,
including sensitivity-to-change, is needed in hand OA and its subgroups.
To cite this abstract in AMA style:
Damman W, Liu R, Kortekaas MC, Rosendaal FR, van der Heijde D, Kloppenburg M. Construct Validity of the Doyle Index in the Outcome Domain of Joint Activity in Hand Osteoarthritis Patients [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/construct-validity-of-the-doyle-index-in-the-outcome-domain-of-joint-activity-in-hand-osteoarthritis-patients/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/construct-validity-of-the-doyle-index-in-the-outcome-domain-of-joint-activity-in-hand-osteoarthritis-patients/