Session Information
Date: Tuesday, October 23, 2018
Title: 5T108 ACR Abstract: RA–DX, Manifestations, & Outcomes V: Outcomes Measures (2868–2873)
Session Type: ACR Concurrent Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: We have previously reported an evaluation of 941 US Veterans in the Veterans Affairs (VA) Rheumatoid Arthritis (RA) (VARA) registry that 559 (59%) did not have a major therapeutic change (MTC) in RA therapy despite elevated DAS28>3.2. Medical chart notes found that a comprehensive provider judgment (CPJ) of acceptable/low disease activity was a leading factor in the decision to not change therapy despite elevated disease activity by DAS28. This study investigates the utility of CPJ and DAS28 to predict MTC in patients with moderate (DAS28=3.2 to 5.1) and severe (DAS28>5.1) RA and compares types of MTC to determine whether specific changes varied according to the DAS28 and/or CPJ.
Methods: US Veterans in the VARA registry with 1) moderate/severe disease activity (DAS28≥3.2) on index day 2) 18 months of VA data prior to the index date and 3) 90 day observation after index date were eligible for review. A MTC was defined as 1) re-initiation of prior DMARD and/or prednisone (Pred) after ≥90 day gap in therapy, 2) initiation of new DMARD and/or Pred, 3) escalation of current DMARDs and/or Pred and/or 4) 2 joint injections within either 7 days before to 90 days after the index date. There were 403 patients from 9 VARA registry sites meeting the above criteria randomly selected for chart review. A CPJ was made by the chart reviewer (JS) blinded to DAS28 who categorized CPJ as mild or moderate/severe on the basis of text notes by the provider using these terms or similar comments on disease state. The MTC decisions were then stratified by the corresponding CPJ and DAS28 levels to investigate their association with MTC. Specific MTC actions were classified as joint injection, gaps in therapy with re-initiation of same DMARD for Pred, or initiation new DMARD or Pred/escalation of current DMARD or Pred.
Results: The 403 patients evaluated were age 65±10 years, RA disease duration 14±11 years, 85% male, 81% seropositive for rheumatoid factor, and 64% positive for aCCP. The proportion of patients with high CPJ with MTC was 124/195 (63.5%) and similar to MTC in patients with high DAS28 46/72 (64.8%) The interaction of CPJ and DAS28 on MTC suggests CPJ may have a higher association with MTC than DAS 28 (Figure). When evaluating the specific types of MTC that occurred in the groups stratified by both CPJ and DAS28 there were no evident differences in the types of changes that were instituted (Table).
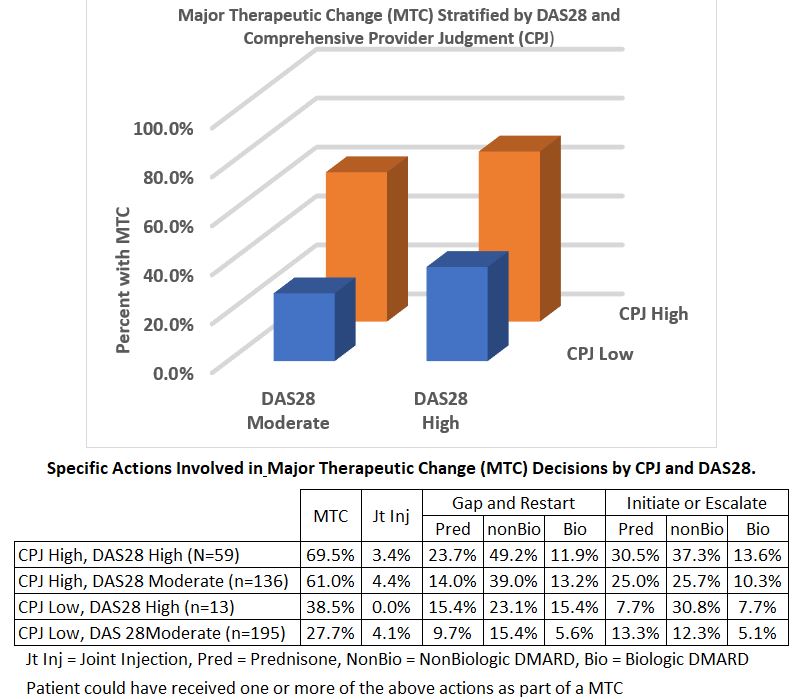
Conclusion: Less than half of patients (45.5%) studied received a MTC despite having moderate to severe RA by DAS28. High disease activity by either CPJ or DAS28 were associated with MTC. In patients with moderate DAS28, a high CPJ was associated with a greater tendency to have a MTC. The specific actions involved in the MTC did not vary significantly with CPJ or DAS28 levels. Both CPJ and the DAS28 appear to be important in the decision to make a MTC in RA patients with moderate/severe disease activity by DAS28.
To cite this abstract in AMA style:
Stever JR, Sauer BC, Cannon GW. Comprehensive Provider Judgement Is a Significant Determinant of Major Therapeutic Change in Patients with Moderate to Severe Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/comprehensive-provider-judgement-is-a-significant-determinant-of-major-therapeutic-change-in-patients-with-moderate-to-severe-rheumatoid-arthritis/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comprehensive-provider-judgement-is-a-significant-determinant-of-major-therapeutic-change-in-patients-with-moderate-to-severe-rheumatoid-arthritis/