Session Information
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Timely initiation of DMARDs in rheumatoid arthritis (RA) is necessary to prevent significant morbidity and mortality. Yet, patients from marginalized groups are less likely to be prescribed these medications. Prior comparisons of faculty and fellows’ clinics show delays in beginning DMARDs in patients at risk for health disparities (HD). This suggests provider-level contributions to HD given these rheumatologists were within the same healthcare system. Therefore, we sought to compare DMARD, biologic, and steroid prescribing patterns between faculty and fellows’ clinics in our urban, minority-majority setting to determine if our fellow and faculty prescribing practices aligned with one another.
Methods: Montefiore Medical Center records were queried for patients with incident RA based on ICD 9 and 10 codes. Diagnosis was verified by a rheumatology visit and documented positive anti-CCP >20 U/mL and/or anti-RF >12 IU/mL antibodies. Those diagnosed with RA prior to the 2012 “Treat-to-Target” recommendations, diagnosed by an outside rheumatologist, or without prescription data were excluded. Status of diagnosing rheumatologist as fellow or faculty, patient demographics, insurance status and SES score (developed by Diez Roux et. al.) were documented. Date of initial visit and length of time until first steroid, DMARD, and biologic prescription were recorded. Statistical analyses included two-sample t-tests, Wilcoxon tests, Chi-square tests, and logistic and Cox regression models.
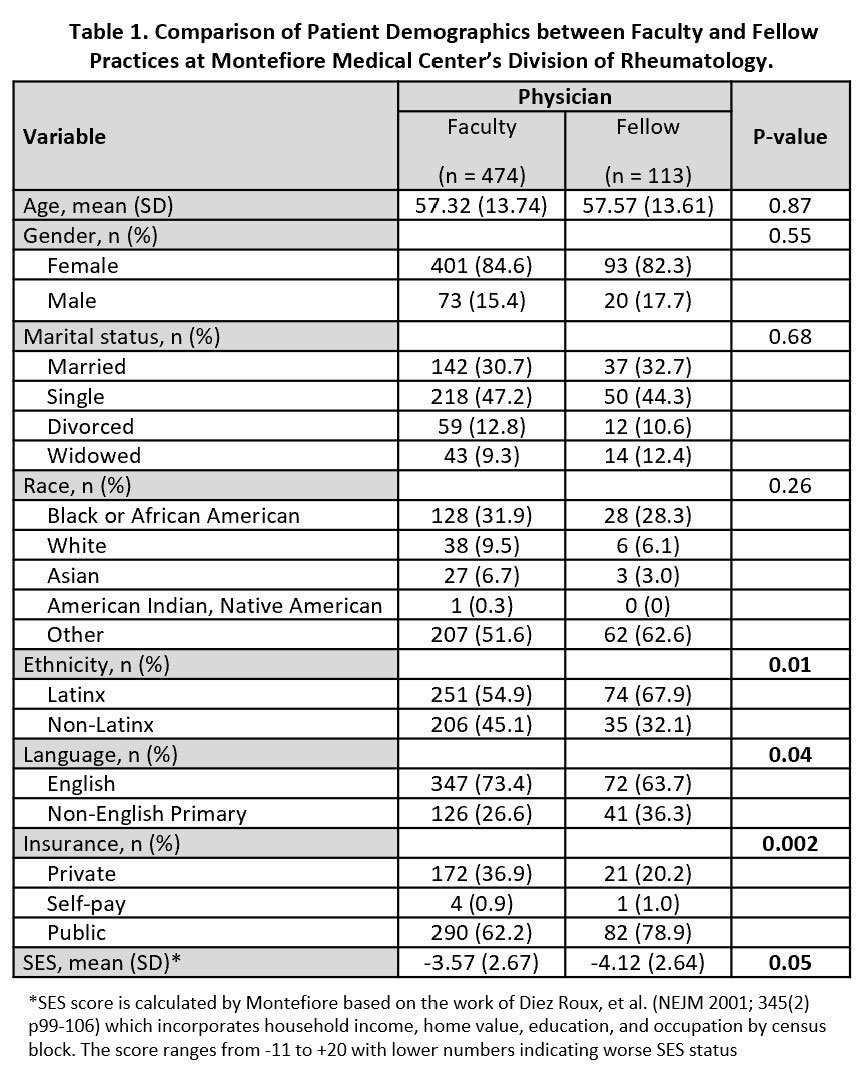
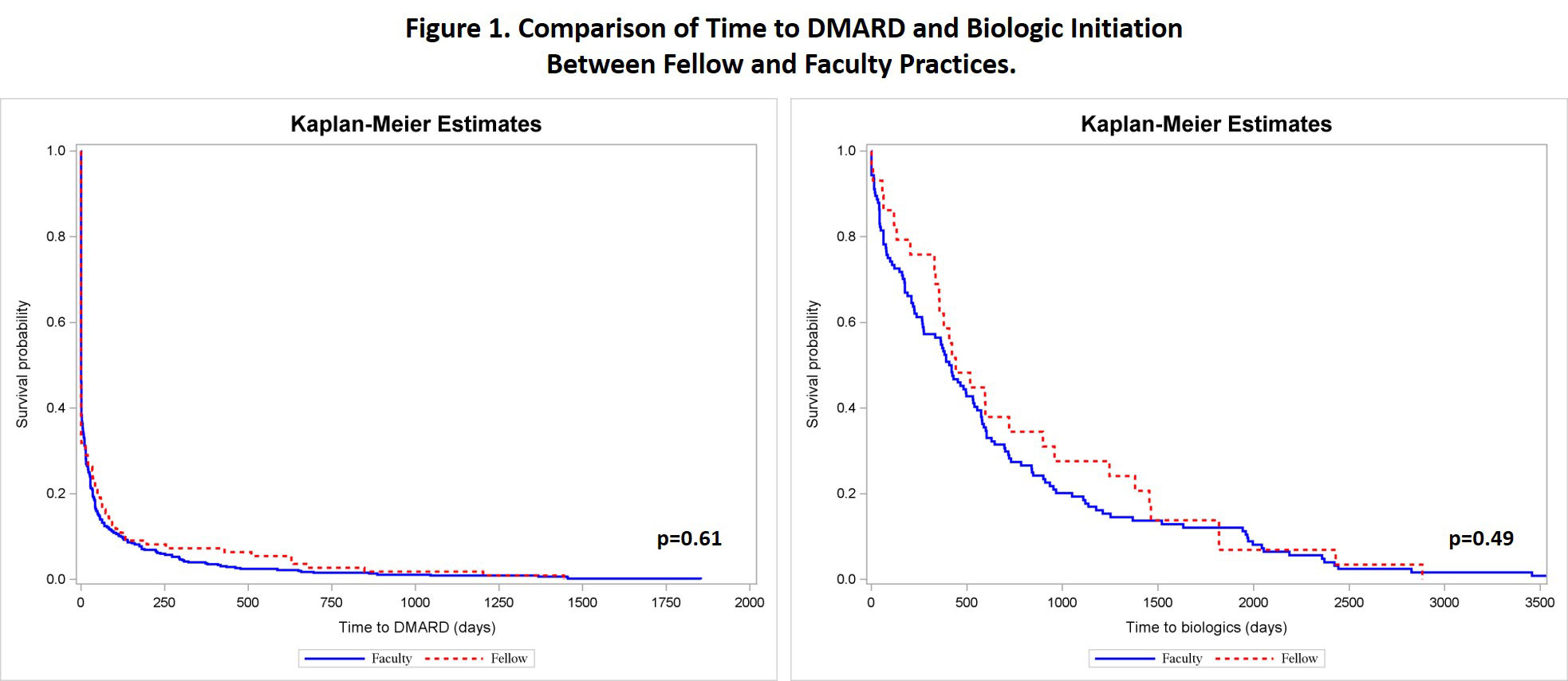
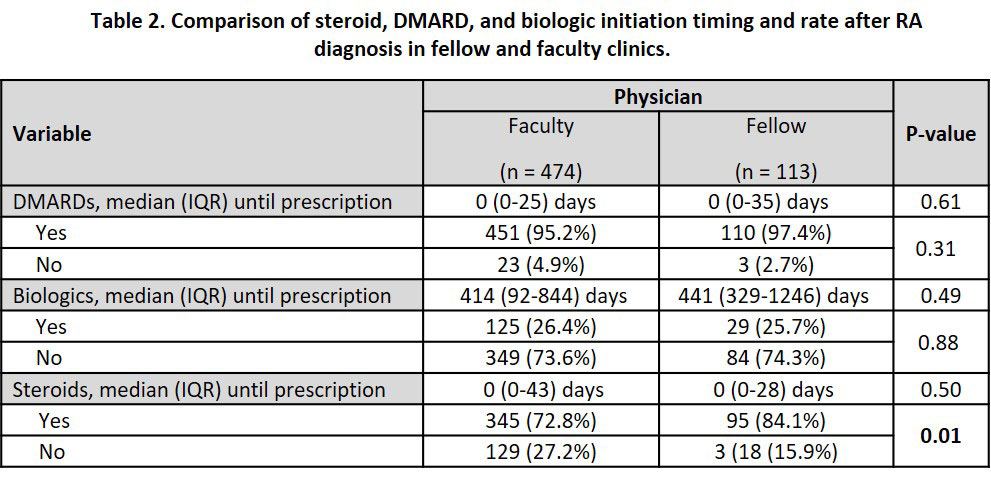
Results: Of 587 Bronx-based RA patients, 113 were seen by fellows and 474 were seen in a faculty practice. Both groups had a similar distribution of age, gender, marital status, and race. Fellows saw more Latinx patients and patients whose primary language was not English (p=0.01, p=0.04). Patients seen by both fellows and faculty were of low SES, but those seen by fellows had lower SES scores and were less likely to have private insurance (p=0.05, p=0.002) (Table 1). Both faculty and fellows had a median time to DMARD prescription of 0 days (p=0.61). The median time to biologic initiation was also similar among the groups despite fellows having a wider range of initiation times (p=0.49) (Figure 1). The teaching practice prescribed steroids to 84.1% of patients while faculty prescribed steroids to 72.8% patients despite similar timing of steroid initiation (p=0.01, p=0.50) (Table 2). Even after adjusting for race, ethnicity, primary language, insurance, and SES, the fellows had higher rates of steroid use although similarities in DMARD and biologic initiation remained.
Conclusion: Our faculty and fellows practice in an ethnically diverse, urban health system. Though fellows had slightly more disadvantaged patients, both fellows and faculty had excellent rates for DMARD and biologic initiation. It is possible that because faculty also saw disadvantaged patients, this allowed them to teach fellows how to address the needs of these patients. Nevertheless, differences in steroid prescribing patterns by fellows, despite faculty mentoring, adds evidence that addressing health disparities at the provider-level is imperative to improve RA outcomes in communities of color and lower SES.
To cite this abstract in AMA style:
Valle A, Xie X, Jackson D, Blanco I. Comparison of Faculty and Fellow Prescribing Patterns for Rheumatoid Arthritis in an Urban, Academic Hospital [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/comparison-of-faculty-and-fellow-prescribing-patterns-for-rheumatoid-arthritis-in-an-urban-academic-hospital/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparison-of-faculty-and-fellow-prescribing-patterns-for-rheumatoid-arthritis-in-an-urban-academic-hospital/