Session Information
Date: Saturday, November 6, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster I: Cardiovascular Pulmonary Disease (0268–0295)
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Compare factors associated with interstitial lung disease (ILD) progression determined on CT-scan analysis and survival in two distinct populations, patients with rheumatoid arthritis associated interstitial lung disease (RA-ILD) and patients with idiopathic pulmonary fibrosis (IPF).
Methods: RA and IPF patients with ILD confirmed by 2 CT-scans spaced from 6 or more months apart (T0: first CT chest scan describing ILD; Tx: last CT chest scan available) were consecutively included in this retrospective multicenter study from 2010 to 2020. CT-scans were blindly analyzed for each patient at T0 and Tx by 2 independent radiologists to determinate ILD pattern (definite usual interstitial pneumonia (UIP), probable UIP, indeterminate UIP, non-UIP) and progression during the follow-up (progressive or stable ILD) defined by the variation of the fibrosis score. Characteristics of patients (demographic-clinical-biological findings, pulmonary function tests, and treatments exposure) at T0 and during the follow-up (T0-Tx) were analyzed as potential determinants of ILD progression through multivariable logistic regression analysis. Overall survival was analyzed using Kaplan-Meier method.
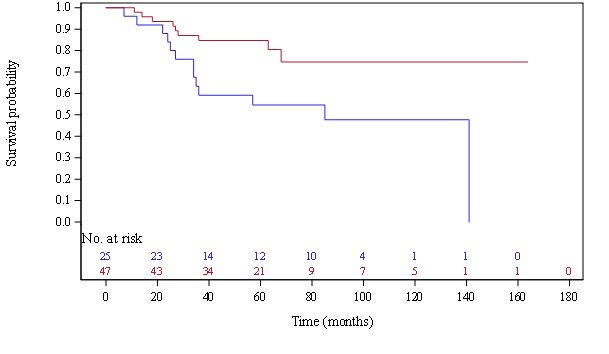
Results: 74 RA-ILD patients and 70 IPF patients were included. During a T0-Tx follow-up of 2.8 ± 2 years, ILD progression was identical in the two populations, of 36%. RA-ILD patients and IPF patients were comparable in terms of age, sex, BMI, smoking history, and severity of initial pulmonary function tests, but T0 CRP rate was higher in RA-ILD patients (29 ± 36mg/L vs 9 ± 35mg/L; p< 0.0001) and T0 CT damage was slightly more pronounced in RA-ILD patients (T0 fibrosis score=27% vs 21%; p=0.05). Multivariate analysis identified different risk factors for ILD progression in the 2 populations. A treatment by Methotrexate at ILD diagnosis was associated negatively with ILD progression in RA-ILD patients (OR=0.14 [0.04-0.52]; p=0.0031) while UIP pattern was positively associated with ILD progression (OR=12 [4.38; 39.85], p=0.0001). In IPF patients, pulmonary comorbidities (OR=8.4 [1.4; 51.4], p=0.02) and the need to oxygen therapy during T0-Tx (OR=5.2 [1.2-22.3], p=0.03) were poor prognosis factors. The follow-up to death or end of collection (July 2020) was longer in RA-ILD patients (5.1 years vs 3.8; p=0.001) but survival rate was not significantly different (31% in RA-ILD patients vs 38 % in IFP patients; HR=1.59 [0.89; 2.84], p=0.1) and better for stable ILD than for progressive ILD in both RA-ILD and IPF populations.
Conclusion: We did not identify any common risk factors for ILD progression in RA-ILD and IPF patients, but in both populations, about one third of patients had ILD progression and died.

To cite this abstract in AMA style:
Lucas C, Tremblay A, Lapotre T, Jouneau S, Lederlin M, Perdriger A. Comparison of Factors Associated with CT-Scan Progression of Interstitial Lung Disease in Rheumatoid Arthritis and Idiopathic Pulmonary Fibrosis. Retrospective Multicenter Study of 144 Patients [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/comparison-of-factors-associated-with-ct-scan-progression-of-interstitial-lung-disease-in-rheumatoid-arthritis-and-idiopathic-pulmonary-fibrosis-retrospective-multicenter-study-of-144-patients/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparison-of-factors-associated-with-ct-scan-progression-of-interstitial-lung-disease-in-rheumatoid-arthritis-and-idiopathic-pulmonary-fibrosis-retrospective-multicenter-study-of-144-patients/