Session Information
Date: Monday, October 27, 2025
Title: (1467–1516) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The Physician Global Assessment (PGA) is used to measure disease activity on a 0–10 scale for many pediatric rheumatic conditions. However, the thresholds at which 0-10 PGA scores correspond to clinically defined categories (inactive, mild, moderate, severe), or a 0-3 scale as utilized in childhood lupus low disease activity state (cLLDAS), are not standardized. Understanding the relationship between 0–10 and 0–3 PGA may clarify if the 0–3 scale is necessary for cLLDAS or whether a transformed 0–10 scale could serve as an acceptable substitute. Our objective was to define 0-10 PGA score thresholds that correspond to clinician-assigned categorical disease activity levels using statistical modeling and predicted probabilities.
Methods: We analyzed electronic health record (EHR) data collected from a tertiary care pediatric rheumatology clinic between December 2021 and February 2023. We identified ambulatory visits for SLE using a clinician-documented structured field. Our EHR documentation included structured fields to collect: 1) 0-10 PGA (21 points with 0.5 increments), built as a drop-down menu; 2) a categorical “Disease Activity Assessment” with radio buttons for “Inactive”, “Mild”, “Moderate”, and “Severe” arranged in a row, representing 0-3 PGA anchored values. We calculated descriptive statistics for PGA by clinician-assigned disease activity category. PGA was then evaluated as a continuous predictor of disease activity category using ordinal logistic regression. Predicted probabilities of each disease activity category were estimated using margins from the ordinal model. We then derived PGA thresholds and calculated the frequency of visits within each PGA category compared to clinician-assigned categories.
Results: We analyzed 190 visits < ![if !supportAnnotations] >[ES1]< ![endif] > < ![if !supportAnnotations] >[LT2]< ![endif] > < ![if !supportAnnotations] >[MM3]< ![endif] > for SLE with both 0-10 PGA and disease activity category completed (Figure 1). Clinician-assigned categories were Inactive for 50% of visits (PGA median 0, IQR 0-0), Mild 42% (1.0, 1-2), and Moderate 8% (3.75, 2.25-5). Each 1-point increase in PGA more than doubled the odds of being assigned to a higher disease activity category (OR = 2.08, 95% CI: 1.57–2.59, p < 0.001). Visits with PGA ≤0.5 had >80% probability of clinician-assigned inactive category, 1-3.5 had the highest probability of mild, and ≥5 had >95% probability of moderate (Table 1). PGA 0-0.5 identified 94% of the visits assigned inactive, 1-3.5 identified 83% of the visits assigned mild, and 4-10 identified 50% of the visits assigned moderate (Table 2),
Conclusion: In children with SLE, 0-10 PGA scores are strongly aligned with clinician-assigned disease activity categories, supporting transformation between the 2 scales. Using a 21-point 0-10 PGA scale, we propose that 0-10 PGA ≤3.5 corresponds to cLLDAS criteria and 0-10 PGA ≤0.5 corresponds to clinical remission criteria, suggesting a modification from strict mathematical transformation. Aligning the cLLDAS 0-3 PGA scale to 0-10 scale used in other pediatric rheumatic conditions is likely to increase reliability of collection in routine clinical practice.
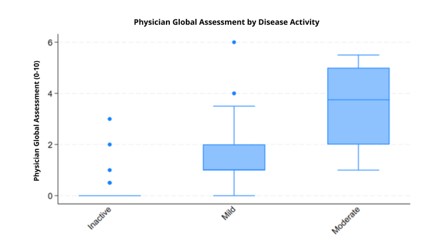 Figure 1. Distribution of 0-10 Physician Global Assessment Scores by Clinician-Assigned Disease Activity Assessment Category (inactive, mild, moderate) across 190 Pediatric Rheumatology Encounters for SLE.
Figure 1. Distribution of 0-10 Physician Global Assessment Scores by Clinician-Assigned Disease Activity Assessment Category (inactive, mild, moderate) across 190 Pediatric Rheumatology Encounters for SLE.
.jpg) Table 1. Predicted Probability of Clinician-Assigned Disease Activity (PGA) Category by 0-10 Physical Global Assessment (PGA) Score
Table 1. Predicted Probability of Clinician-Assigned Disease Activity (PGA) Category by 0-10 Physical Global Assessment (PGA) Score
.jpg) Table 2. Number of visits within each Physician Global Assessment (PGA) Threshold cross-tabulated with Clinician-Assigned Disease Activity Category
Table 2. Number of visits within each Physician Global Assessment (PGA) Threshold cross-tabulated with Clinician-Assigned Disease Activity Category
To cite this abstract in AMA style:
Timmerman L, Mannion M, Smitherman E. Comparing the 0-10 Physician Global Assessment Scale to Categorical Disease Activity States among Pediatric Patients with SLE [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/comparing-the-0-10-physician-global-assessment-scale-to-categorical-disease-activity-states-among-pediatric-patients-with-sle/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparing-the-0-10-physician-global-assessment-scale-to-categorical-disease-activity-states-among-pediatric-patients-with-sle/