Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Rheumatoid Arthritis (RA) is a chronic autoimmune disease with persistent synovial inflammation. Several bDMARDs and tsDMARDs target different key players in the immune-regulatory pathways, including cytokines, JAK, T cells, and B cells. These molecules enable the achievement of remission or LDA in the majority of patients. However, about 20% to 40% of patients fail to achieve remission, and a smaller percentage, recognized as (multi-drug resistance) MDR-RA, fail several bDMARDs and tsDMARDS. In this subset of severe and multi-resistant patients, the combination of a TNFi and a JAKi might be a promising approach, despite not risk-free.
Methods: We performed a descriptive study of patients from the RA UCLouvain Brussels Cohort, who received a combination of TNFi and JAKi. Disease activity trajectory and tolerability, as well as different therapeutic agents received over time, were recorded.
Results: We report five patients (3F, 2M). They received a combination therapy after a median time of 184 months (IQR 116) from diagnosis. The demographic and clinical features for each patient are reported in Table 1. Figure 1 shows disease activity at the moment of each b/tsDMARDs discontinuation (A), reason for discontinuation (B), and the sequence of the b/tsDMARDs (C) for each patient. All of these pts were refractory to 7 bDMARDs and to 2 JAKi. Of note, all the patients received csDMARDs alongside b/tsDMARDs. Variable-dose glucocorticoids have been part of the therapeutic strategy in combination with standard therapy. None of the patients suffered from major adverse events due to b/tsDMARDs as severe infection. All the patients were treated with a TNFi (infliximab or etanercept) associated with a JAKi (Upatacitinib or Filgotinib). Three patients had a minimum follow-up time of 3 months after the combination and then a second evaluation. Pt 1 achieved a persistent remission state up to 3 years of follow-up. We observed a significant decrease in disease activity in two patients, reaching disease remission. None of the patients developed major side effects, including severe infection or hospitalisation, in the observation period.
Conclusion: Our preliminary results indicate that a combination therapy of a TNFi and a JAKi provided good clinical results without safety concerns. In severe and multi-resistant patients, when all classical approach fails to reach a good disease control, the combination therapy could be an option. As infection is the major risk for those patients, a b/tsDMARDs combination should be restricted to young patients with a low infection risk and after adequate vaccinations.
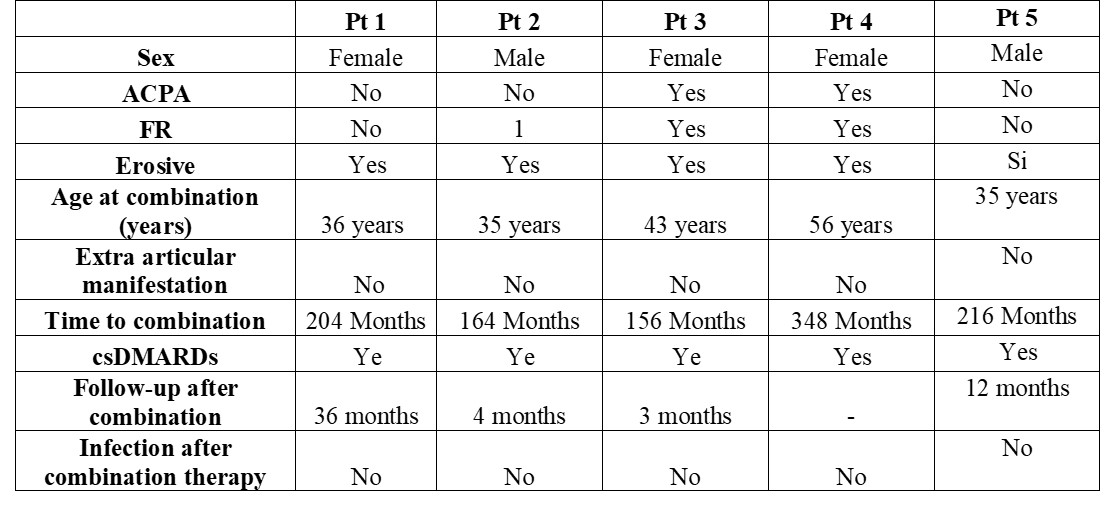 Figure 1 A-D
Figure 1 A-D
A. Disease activity for each patient according DAS28 disease activity score before starting combination therapy (left) and after initiation of combination therapy (right).
B. Reason for discontinuation for each b/tsDMARDs. From the 5th b/tsDMARDs on, only 3 patients are considered.
C. b/tsDMARDs prescription progression for each patient.
D. Glucocorticoid dosage at each b/tsDMARD change
.jpg) Table 1. Demographic and disease feature for each patient
Table 1. Demographic and disease feature for each patient
To cite this abstract in AMA style:
NATALUCCI F, VAN MULLEM C, AVRAMOVSKA A, SOKOLOVA T, Durez P. Combination Therapy with TNF Inhibitors and JAK Inhibitors in Multi-Drug-Resistant Rheumatoid Arthritis: A Case Series from the RA UCLouvain Brussels Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/combination-therapy-with-tnf-inhibitors-and-jak-inhibitors-in-multi-drug-resistant-rheumatoid-arthritis-a-case-series-from-the-ra-uclouvain-brussels-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/combination-therapy-with-tnf-inhibitors-and-jak-inhibitors-in-multi-drug-resistant-rheumatoid-arthritis-a-case-series-from-the-ra-uclouvain-brussels-cohort/