Session Information
Date: Tuesday, November 14, 2023
Title: (1913–1944) Miscellaneous Rheumatic & Inflammatory Diseases Poster III
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: VEXAS (vacuoles, E1 activating enzyme, X-linked, auto-inflammatory, somatic) syndrome is a clinically serious and potentially fatal adult-onset disease caused by somatic mutations in the UBA1 (Ubiquitin-like modifier activating enzyme 1) gene in hematopoietic progenitor cells. VEXAS syndrome clinically presents with inflammatory and hematological symptoms in middle and older age, predominantly in males. Multisystem inflammation most commonly affects the skin, eyes, joints, blood vessels, cartilage, and lungs. Patients with VEXAS syndrome may meet diagnostic criteria for several rheumatic diseases and/or hematological disorders. Given its heterogeneous clinical manifestations a high degree of clinical suspicion is required for pursuing the diagnosis of VEXAS syndrome; therefore, clinicians must be aware of the clinical features of VEXAS syndrome. The purpose of this study is to describe a series of cases diagnosed in a rheumatology department.
Methods: Institute of Rheumatology is the largest tertiary academic center providing care for patients with all types of inflammatory rheumatic diseases in the Czech Republic. Patients with symptom onset at age ≥40 years with undiagnosed inflammatory conditions, chondritis, unclassified vasculitis, neutrophilic dermatosis and classifiable inflammatory rheumatic diseases, which were a) resistant to standard therapy, b) associated with hematologic disorders or c)associated with atypical inflammatory manifestations for given diagnosis were considered for UBA1 testing. Retrospective chart review was performed to obtain pertinent demographic information and clinical data for patients with detected UBA1 somatic mutations.
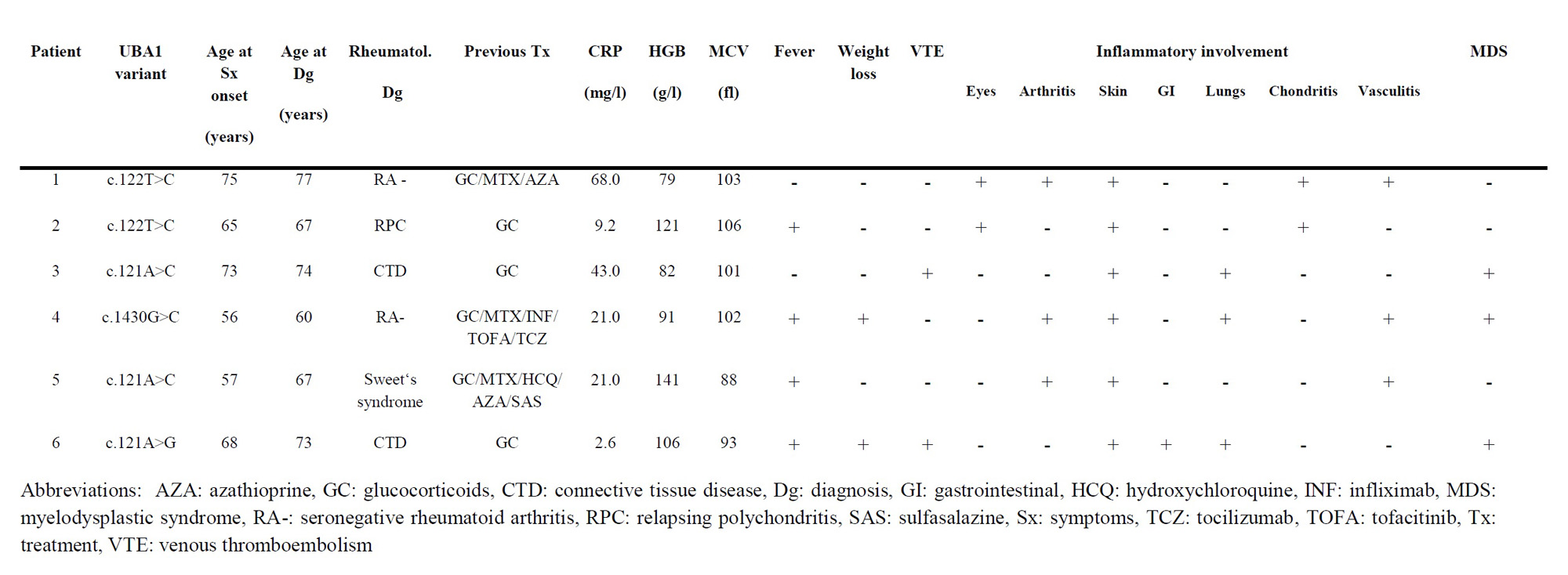
Results: We have tested 22 patients (17 males and 5 females) with suspicious clinical phenotype and were able to detect previously described somatic UBA1 mutations in five of them. One additional patient with clonal cytopenia and multi-organ inflammatory features (patient 4) harbored a previously undescribed UBA1 variant in exon 14, which proved pathogenic in enzymatic analyses (1). Clinical features of individual patients are summarized in Table 1. All patients were males with a median age at symptom onset 66.5 years (IQR 57, 73) and median duration of symptoms prior to VEXAS syndrome diagnosis 3 years (IQR 2, 5). All patients were treated for a presumptive rheumatologic diagnosis with glucocorticoids and three patients received various other immunosupressants prior to the diagnosis of VEXAS syndrome. Myelodysplastic syndrome was diagnosed based on bone marrow biopsy in three patients, two additional patients had macrocytic anemia. Notably no cytopenia and normal MCV were present in one patient with longstanding inflammatory symptoms.
Conclusion: VEXAS syndrome presents with heterogenous clinical manifestations and should be considered in rheumatology patients with corresponding inflammatory phenotype even in the absence of hematologic abnormalities. 1) Stiburkova B, et al.Novel Somatic UBA1 Variant in a Patient With VEXAS Syndrome. Arthritis Rheumatol. 2023 Feb 10. doi: 10.1002/art.42471. Epub ahead of print.
Supported by Ministry of Health of the Czech Republic, grant nr. NU23-10-00160
To cite this abstract in AMA style:
Mann H, Stiburkova B, Pavelcova K, Belickova M, Salek C, Juhaszova J, Vencovsky J. Clinical Spectrum of VEXAS Syndrome in a Rheumatology Department [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/clinical-spectrum-of-vexas-syndrome-in-a-rheumatology-department/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-spectrum-of-vexas-syndrome-in-a-rheumatology-department/