Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Adult Onset Still’s Disease (AOSD) is a rare systemic inflammatory disorder characterized by inflammatory polyarthritis, daily fever, and a transient salmon-pink maculopapular rash. Diagnosis of AOSD is challenging as patients may have a variety of non-specific symptoms and laboratory abnormalities, and diagnosis is often exclusionary due to the ambiguous nature of its presenting symptoms. Interleukin 18 (IL-18) levels have been found to be markedly elevated in AOSD patients,1 and present a promising indicator for disease activity and diagnosis. We aimed to describe a cohort of AOSD patients, including their serum IL-18 levels and treating rheumatologist-reported disease activity, as seen in outpatient clinic visits at a tertiary care referral hospital in the United States.
Methods: We enrolled adult patients (≥18 years) with AOSD in a prospective cohort. Patients were identified by ICD-10 codes (M06.1). Clinical diagnosis of AOSD was then confirmed with the patients’ respective treating rheumatologists, and subsequently via chart review by a second rheumatologist who oversees a specialized AOSD practice. Patients with a different disease that explained the clinical picture better than AOSD were excluded. Demographic data, medication use, medical history, and laboratory results were collected via chart review. Patients were characterized using three standard AOSD diagnostic criteria – Yamaguchi, Cush, Fautrel – and descriptive statistics were reported.
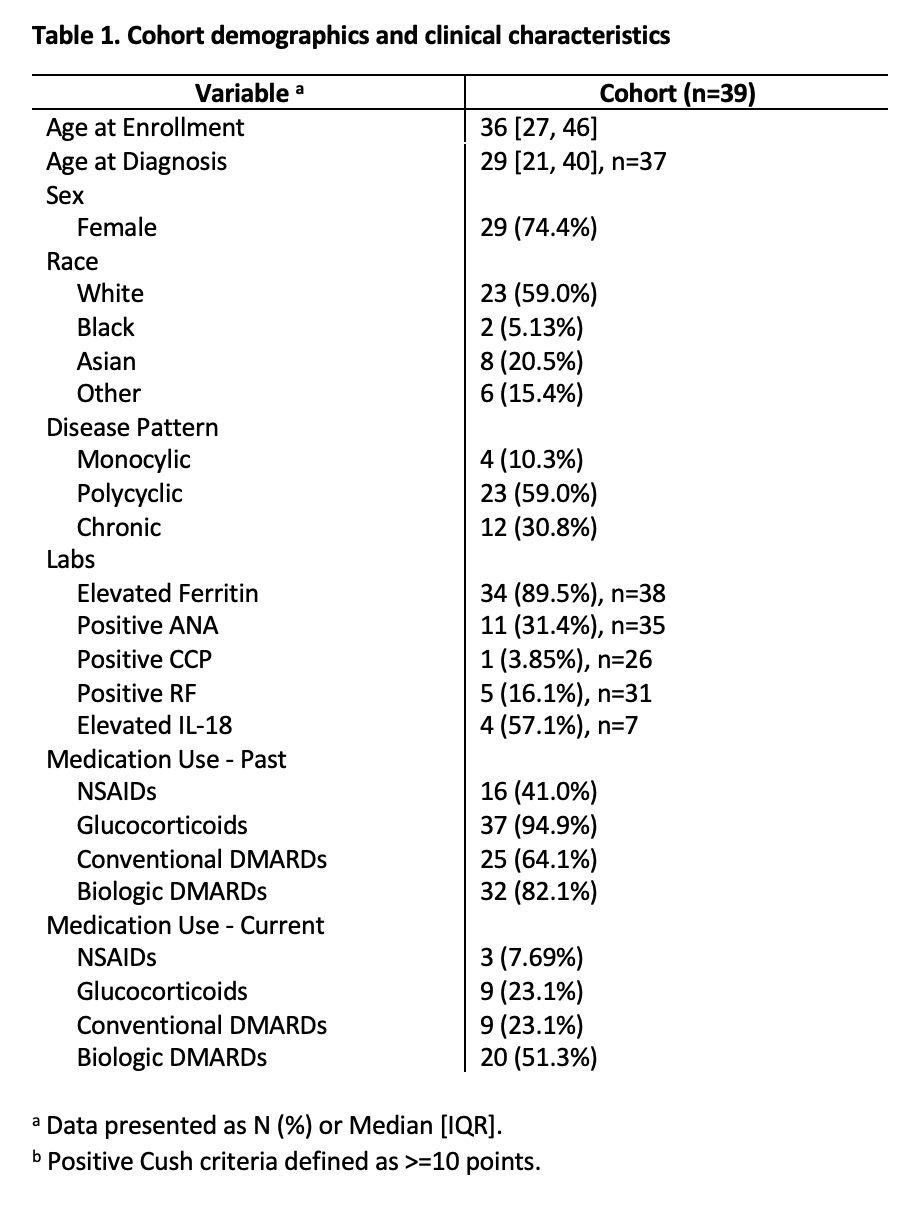
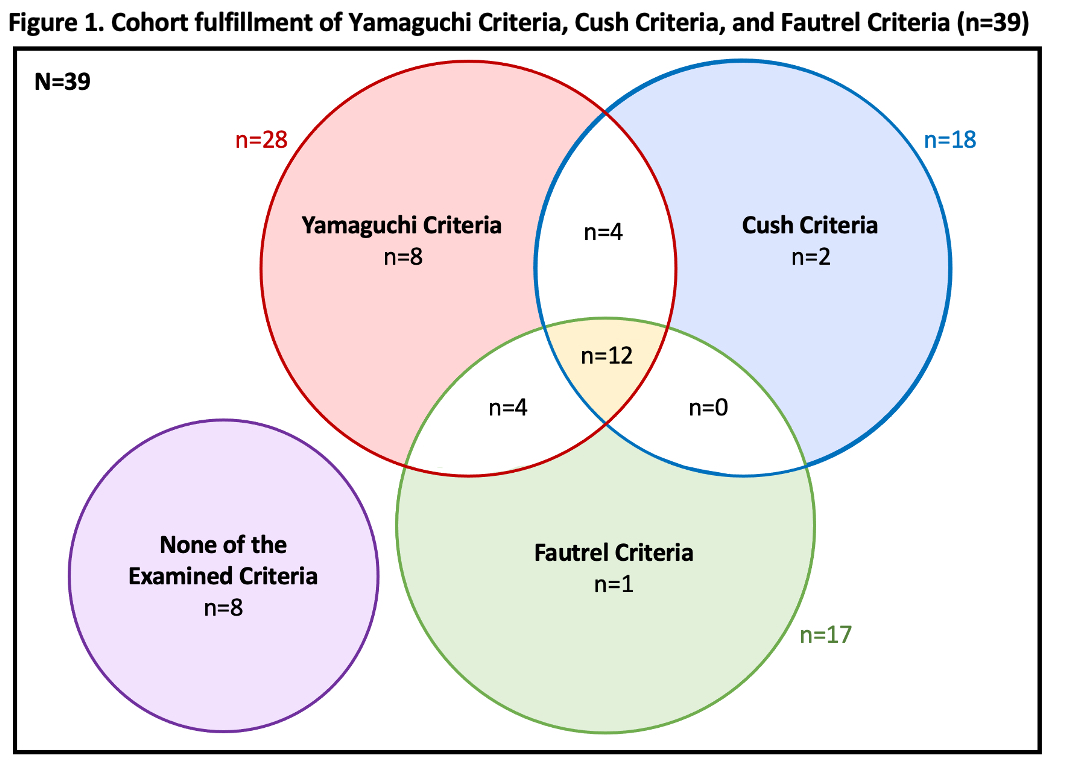
Results: 39 patients were enrolled, majority White (59.0%) and female (74.4%) (Table 1). Of the examined diagnostic criteria, only 30.8% of patients met all three and 20.5% fit none (Figure 1). All patients were treated clinically as AOSD despite differences in fulfilling diagnostic criteria.
23.6% of patients had a history of macrophage activation syndrome (MAS). Peak ferritin levels were markedly elevated in the cohort (median 2102.5 ng/mL, IQR [445, 10798], n=38). 12 patients presented with elevated peak ferritin levels >10,000 ng/mL, including 6 with history of MAS.
Serum IL-18 levels were measured in 7 patients (median 554 pg/mL, IQR [246.5, 36151]), and were elevated in 4 patients whose treating rheumatologists noted worsening of clinical symptoms at time of measurement.
Conclusion: We characterized a cohort treated clinically as AOSD and identified that 20.5% did not fit any diagnostic criteria while only 30.8% met all three. It is imperative to recognize that not all patients neatly fit into established criteria, and patients may be excluded depending on which criteria was selected, highlighting the heterogeneity of the disease. Serum IL-18 levels were only measured in a portion of our cohort, but we observed an association between elevated serum IL-18 levels and worsening symptoms as noted by the treating rheumatologist. Continued disease characterization and measurement of serum IL-18 levels in AOSD patients, especially to further elucidate its potential role in AOSD diagnosis, is necessary in rare diseases where traditional diagnostic criteria may not be the clinical reality.
1. Colafrancesco et al. IL-18 Serum Level in Adult Onset Still’s Disease: A Marker of Disease Activity. PMID: 22762008.
To cite this abstract in AMA style:
Heiting C, Gambina K, Mehta B. Clinical Realities in Patients with Adult Onset Still’s Disease: Real-World Diagnosis and Management [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/clinical-realities-in-patients-with-adult-onset-stills-disease-real-world-diagnosis-and-management/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-realities-in-patients-with-adult-onset-stills-disease-real-world-diagnosis-and-management/