Session Information
Date: Sunday, November 13, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster II: Manifestations
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Antiphospholipid Antibody (aPL) are described in 11-40% of patients with SLE. Whether the presence of any of the aPLs or combinations thereof, can accurately predict the risk of thrombosis, non-thrombotic events and obstetric outcome in SLE has been debatable. We report the prevalence, associations and outcomes in SLE patients with aPL.
Methods: From the ongoing prospective INdian SLE inception cohort (INSPIRE) data was extracted for SLE patients for whom complete data was available for all the five routinely performed aPL- lupus anticoagulant (LAC), IgG and IgM isotypes for anticardiolipin antibody(aCL) and anti-β2-glycoprotein-I (β2GPI) at enrolment. Patients were categorised into no aPL, triple positive [positive for all 3; LAC, aCL (IgG and or IgM), anti-β2-GPI (IgG and or IgM)], dual positive (any 2 of 3; LAC / aCL / β2-GPI) and isolated aPL positive. The aPL antibodies methodology and cut offs were as per recommendations (1,2). Patients with thrombotic, non-criteria/ non-thrombotic events (NTE) and obstetric outcomes were analysed for associations and compared against those who were negative for all aPL. Odds ratio (OR) adjusted for age, gender and SLEDAI was calculated for all variables except obstetric manifestations, where OR was adjusted for age and SLEDAI.
1.Update of the guidelines for lupus anticoagulant detection 7(10),1737–1740
2.International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome J.Thromb. Haemost. 2006,4,295–306
Results: We analysed 1023 patients (92.6% women), mean age 28.7 ± 10.1 years including 105(10.3%) children. 36 (3.5%) were identified as triple positive and at least one aPL antibody was detected in 358(35%). Overall, the aPL positive group had significant association with gangrene, myocardial infarction, stroke, 2nd trimester miscarriage, thrombocytopenia and autoimmune hemolytic anaemia (p< 0.05). Fig1
There were 82 thrombotic events in 66 patients (6.5%) in our cohort and thrombotic events were associated with presence of LAC [aOR 1.78(1.0,3.17)] and β2-GPI [aOR 2.23(1.04,4.78)]. Tab 1
There were 984 conceptions in 456 women, averaging 2.1 conceptions per woman. There were 194 obstetric events of interest and were significantly associated with at least one aPL positivity [aOR 1.473(0.98,2.19)]. Low birth weight had high odds with triple positivity [aOR 2.708(1.01,7.39)] and 2nd trimester miscarriages with presence of LAC [aOR 3.213(1.19,8.62)]. Tab 2
Amongst the non-criteria events, AIHA had higher odds of occurrence with LAC [aOR 1.80(1.09,2.97)], dual positivity [aOR 2.18(1.51,3.16)], thrombocytopenia with dual positivity [aOR 2.98(1.85,4.8)] and any NTE with LAC [aOR 1.63(1.01,2.65)]. Tab1
There were 44/1023(4.3%) deaths in this cohort, 22/358(6.1%) in the aPL group and 22/ 665(3.3%) in the non-APS group, hazard ratio being [1.91(1.04,3.51)] in those with at least one aPL positivity and [3.18(1.46,6.87)] in dual positives after adjusting for age, gender and SLEDAI.
Conclusion: Antiphospholipid antibodies are present in nearly one-third of patients in INSPIRE cohort and their presence increases the risk of thrombotic events, adverse foetal outcomes, non- thrombotic events and mortality.
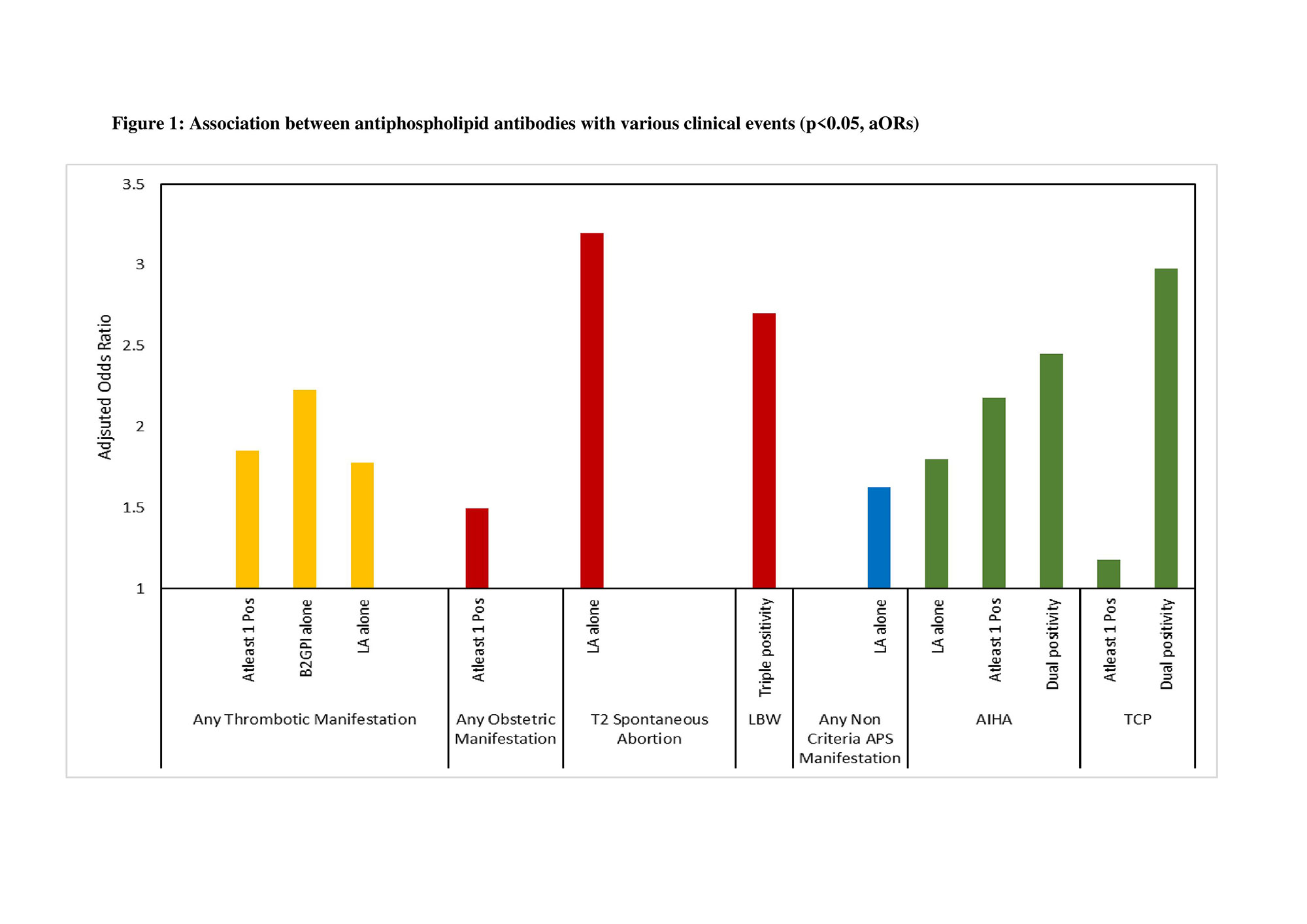
Abbreviation: LA – Lupus Anticoagulant, Pos – Positive, T2 Spontaneous Abortion – Spontaneous Abortion in 2nd Trimester, LBW- Low Birth Weight, APS- Antiphospholipid Syndrome, AIHA- Autoimmune Hemolytic Anemia, TCP- Thrombocytopenia.
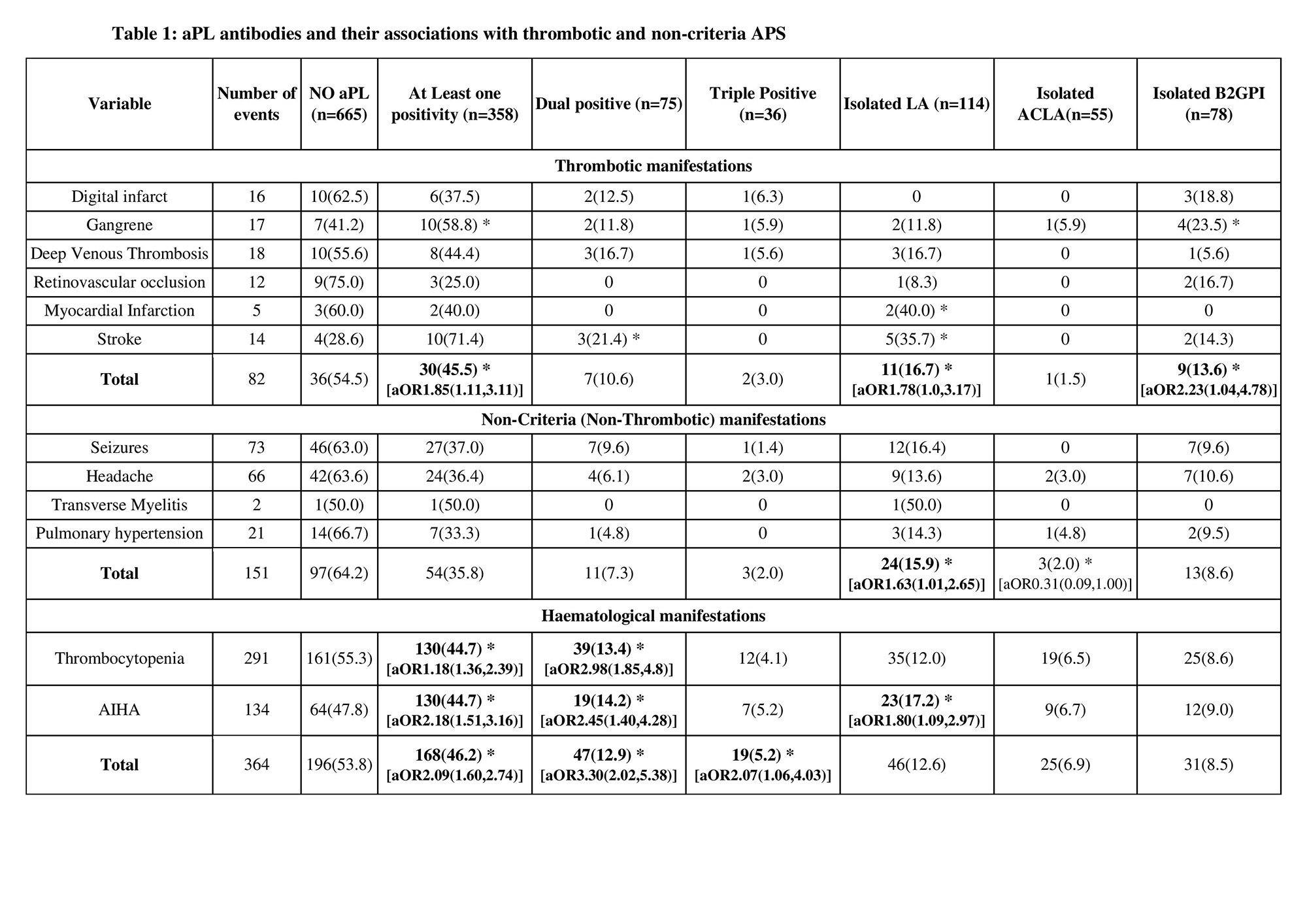
Only significant values are reported, * denotes p<0.05, Adjusted Odds Ratio with confidence Interval denoted as [aOR(C.I)]; adjusted for age and gender and SLEDAI. Abbreviation: AIHA - Autoimmune Hemolytic anaemia, APS - antiphospholipid syndrome.
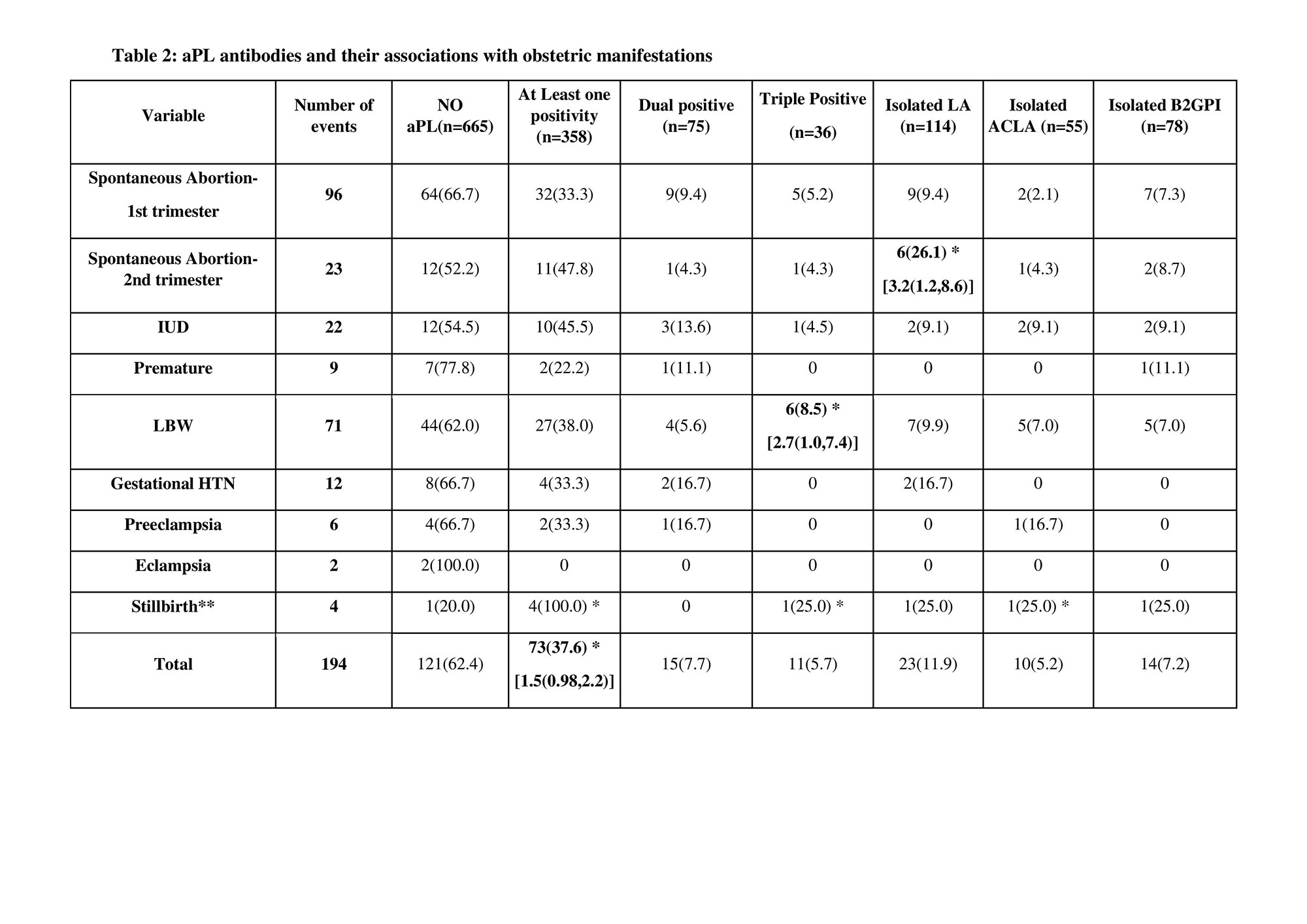
Only significant values are reported, * denotes p<0.05, Adjusted Odds Ratio with confidence Interval denoted as [aOR (C.I)]; adjusted for age and SLEDAI.
**For Stillbirth, aOR is not calculated due to small sample size.
Abbreviation: IUD – Intrauterine death, LBW – Low birth weight, Gestational HTN – Gestational hypertension.
To cite this abstract in AMA style:
Shobha V, Rajasekhar L, Manuel S, Kavadichanda C, Mathew A, Gupta R, Rathi M, Ghosh P, Tripathy S, Jain A, Aggarwal A. Clinical Profiling and Antiphospholipid Antibody (aPL) Associations in Indian Systemic Lupus Erythematosus (SLE) Cohort [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/clinical-profiling-and-antiphospholipid-antibody-apl-associations-in-indian-systemic-lupus-erythematosus-sle-cohort/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-profiling-and-antiphospholipid-antibody-apl-associations-in-indian-systemic-lupus-erythematosus-sle-cohort/