Session Information
Date: Sunday, October 26, 2025
Title: (0233–0279) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: VEXAS syndrome is a rare disease caused by somatic mutations in UBA1 gene. Different mutations in this gene appear to be associated with specific phenotypes, potentially influencing disease severity and progression. This work aims to describe the clinical, phenotypic, and laboratory characteristics of a Spanish cohort of patients with confirmed VEXAS syndrome and to evaluate associations between UBA1 mutations, manifestations and mortality.
Methods: An observational, ambispective study conducted across rheumatology units in Spain, identifying patients with genetically confirmed VEXAS syndrome. Demographic, clinical, laboratory, and outcome data were collected. Statistical analyses were performed using standardized tests (significance set at p < 0.05).
Results: A total of 50 patients with VEXAS syndrome were identified, all male and of Caucasian origin. The mean age at symptom onset was 68.05 years (SD±10.24) and the mean age at diagnosis was 73.49 years (SD±8.72). The mean diagnostic delay was 5.79 years (SD±4.4). “Table 1” summarizes the most common initial misdiagnoses.The most frequent clinical manifestations included cutaneous lesions (88%), arthritis, constitutional symptoms, non-infectious fever, (76% respectively), and chondritis (48%). Other hallmark features of the syndrome, such as pulmonary involvement, thromboembolic disease associated with VEXAS, and renal impairment, were observed in 38%, 32%, and 22% of the patients (see “Table 2”).Laboratory findings revealed anemia in 47 patients (94%), with macrocytosis in 41. The mean hemoglobin level was 9.89 g/dL (SD±2), and the mean MCV was 107.3 fL. Additionally, 23 patients (46%) presented with leukopenia (mean leukocyte count 5337/mm3) and 22 (44%) with thrombocytopenia (mean platelet count 136950/mm3). MDS was present in 44% of the cases, while MGUS was identified in 26% (see “Table 2”). Genetic analysis identified the leucine variant as the most frequent UBA1 mutation (40%, n=20), followed by threonine (36%, n=18) and valine (16%, n=8). Four patients harbored other UBA1 mutations, two of which were classified as VUS (c.1798A >G, p.Thr600Ala and c.209T >A, p.Leu70His), previously unreported. Significant associations were found between leucine and MGUS, threonine and thrombocytopenia, and valine and renal involvement. Non-significant numerical trends included leucine with Sweet’s syndrome (inverse with medium-vessel vasculitis), threonine with thromboembolic disease, and valine with multisystemic involvement (“Image 1”).Mortality occurred in 11 patients (22%), with only 6 deaths (12%) related to VEXAS activity. Periorbital edema was significantly associated with VEXAS-related death (5/6, p=0.006). No significant mortality differences were found between UBA1 variants.
Conclusion: Patients with VEXAS syndrome in this cohort are predominantly older males presenting with cutaneous, constitutional, and articular symptoms, reflecting a “rheumatologic profile”. Specific genotype-phenotype correlations were identified (leucine: MGUS, threonine: thrombocytopenia, valine: renal involvement), along with potential severity markers (periorbital edema: mortality).
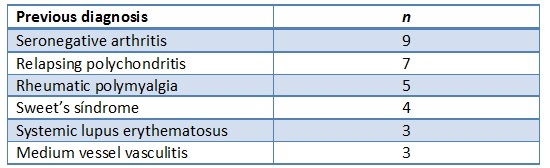 “Table 1”. Most common initial misdiagnoses.
“Table 1”. Most common initial misdiagnoses.
.jpg) “Table 2”. Clinical characteristics and laboratory findings according to main mutations.
“Table 2”. Clinical characteristics and laboratory findings according to main mutations.
.jpg) “Image 1”. Mutations and main clinical associations.
“Image 1”. Mutations and main clinical associations.
To cite this abstract in AMA style:
García-Escudero P, López M, Magallares B, Fiallo Suárez D, Dios Santos D, Egües Dubuc C, Castañeda S, Garcia A, Morante Bolado I, Oliver García E, Garcia Belando C, Corrales C, Toyos F, Font-Urgelles J, Salles Lizarzaburu M, Merino C, Carrion I, Hernandez J, Villalobos L, Boteanu A, Frade Sosa B, Sieiro c, Monjo Henry I, Trallero E, Enriquez E, Rodriguez M, Riera Alonso E, Ibañez M, Reina D, Melero González R, Boselli G, Mariano A, Vázquez Gómez I, Miranda J, Moriano C, Aurrecoechea E, Vela Casasempere P, Rúa-Figueroa I, Calvo J. Clinical Landscape and Severity Markers of VEXAS Syndrome in a Spanish Cohort: Findings from VEXASSER Study Group [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/clinical-landscape-and-severity-markers-of-vexas-syndrome-in-a-spanish-cohort-findings-from-vexasser-study-group/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-landscape-and-severity-markers-of-vexas-syndrome-in-a-spanish-cohort-findings-from-vexasser-study-group/