Session Information
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Takayasu arteritis (TAK) is a rare systemic vasculitis. It occurs most commonly in patients aged < 40 years (y), and 32% of patients present at age < 20 y. Understanding childhood TAK (cTAK) has been limited with studies to date describing small cohorts primarily from single centers. The aim of the study was to characterize disease presentation, early disease course and outcomes within the first 12 months (mo) of disease.
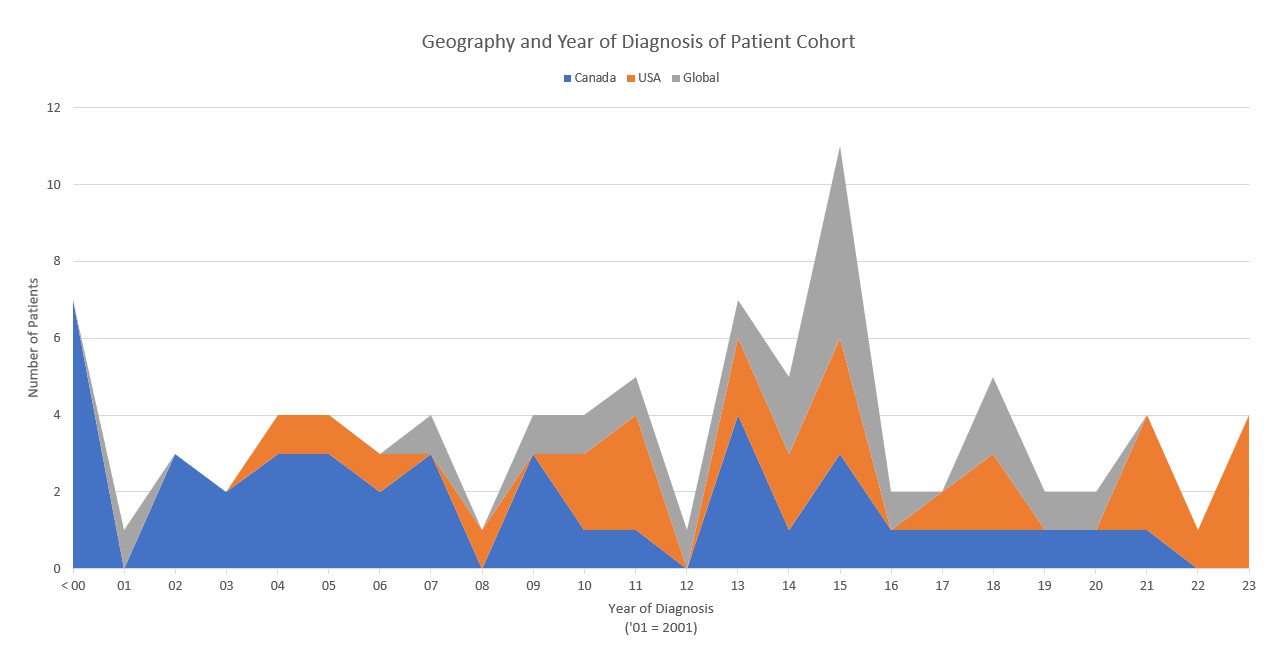
Methods: PedVas is a multicenter, ambispective international registry of clinical data and biological samples from children diagnosed with chronic vasculitis, including cTAK, from 1986 to present. Data collected via Research Electronic Data Capture (REDCap) included presenting clinical features, laboratory results, imaging, treatment, disease activity and damage scores. Disease activity and damage were measured using Pediatric Vasculitis Activity Score (PVAS) and the Pediatric Vasculitis Damage Index (pVDI). A PVAS score of 0 is considered inactive disease and a pVDI of 0 is considered no damage.
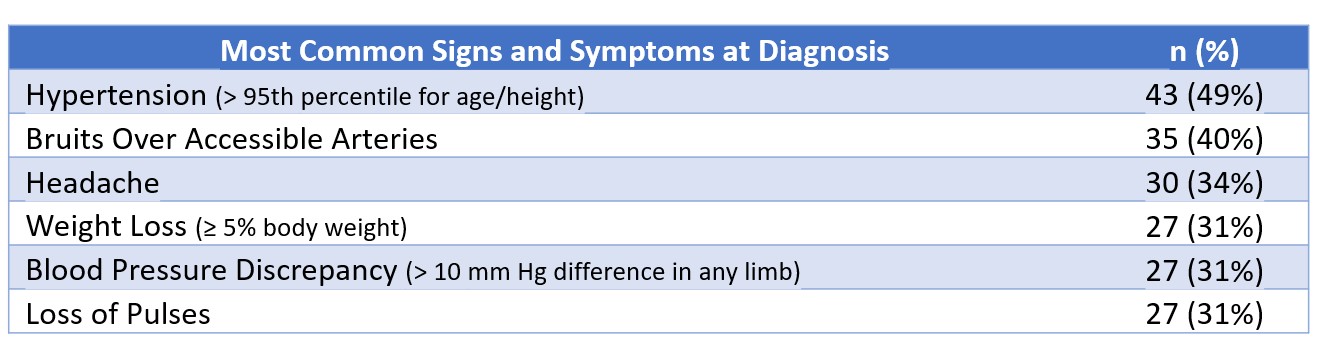
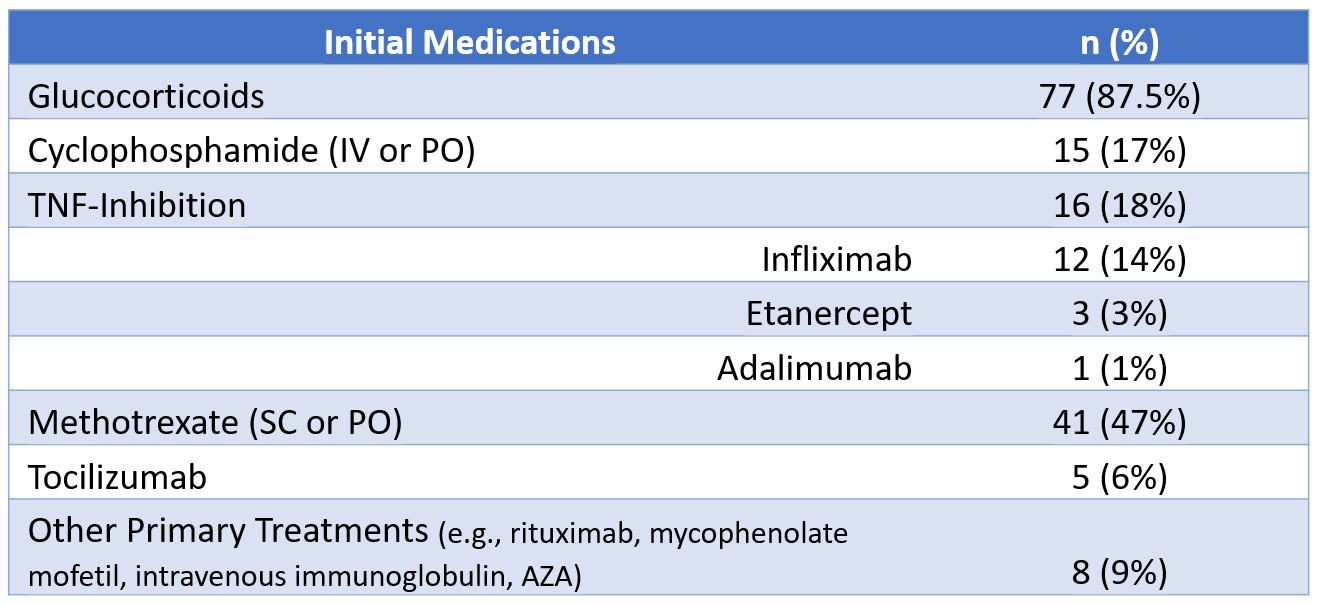
Results: Eighty-eight patients (67% female; median age at diagnosis 12.3 y (interquartile range (IQR) 8.2-15.3) from 11 countries were included in the cohort. Data from 64 patients was available at post-induction visit (3-6 mo after diagnosis), and from 59 at 12 mo. The median time from first symptoms to diagnosis was 2.5 mo (IQR 1-7.25). Table 1 lists the most common signs and symptoms at diagnosis. Initial medications received are shown in Table 2. The descending aorta (58 patients; 66%) and renal arteries (46 patients; 52%) were the vessels most affected, with vessel wall thickening the most reported aortic abnormality. MR Angiography was the most common imaging modality used at time of diagnosis, although many patients had multiple imaging modalities reported.
ESR was elevated ( > 20 mm/hr) in 68% patients at diagnosis; 24% at post-induction; and 22% at 12 mo. CRP was elevated in 61% patients at diagnosis; 18% at post-induction; and 16% at 12 mo. The median PVAS at diagnosis was 10 (IQR 7-16); 1 (IQR 0-3.25) at post-induction; and 0 (IQR 0-2.25) at 12 mo. Fifty-seven percent of patients achieved inactive disease (PVAS = 0) at 12 mo. The median pVDI at 12 mo was 2 (IQR 0-2). Seventy-one percent had sustained some damage at 12 mo (pVDI ≥ 1) with scores of ≥ 5 in 5%, not including 2 patient deaths. Eighty-five percent of patients remained on some amount of glucocorticoid at 12 mo.
Conclusion: Clinical features of cTAK at diagnosis are like those in adults. Glucocorticoid use for induction was widespread but there was no standard approach for use of additional immunosuppressive therapy. Over half of patients achieved inactive disease at 12 mo but a majority remain on GC at that time. Disease damage is common and can be severe in a subset of patients at 12 mo. This study represents the largest, multicenter, international cohort of cTAK ever reported.
To cite this abstract in AMA style:
Bistolarides J, Sivaraman V, Bosman E, Wagner-Weiner L, Morishita K, Nocton J, Liegl M, Pan A, Cabral D. Clinical Features, Treatments, and Outcomes of a Large International Cohort of Childhood-onset Takayasu Arteritis: A PedVas Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/clinical-features-treatments-and-outcomes-of-a-large-international-cohort-of-childhood-onset-takayasu-arteritis-a-pedvas-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-features-treatments-and-outcomes-of-a-large-international-cohort-of-childhood-onset-takayasu-arteritis-a-pedvas-study/