Session Information
Date: Saturday, November 16, 2024
Title: Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Adverse effects of statin use involve the muscle and related rhabdomyolysis. Known risk factors for rhabdomyolysis include female sex, older age, Asian race, hypothyroidism, kidney and liver disease, higher dose of statin medication, and concomitant use of other drugs. We characterized patients who were hospitalized with rhabdomyolysis.
Methods: Data was collected retrospectively from the HCA Healthcare database from 2016 to 2023. Persons over 18 hospitalized for rhabdomyolysis and statin induced myopathy on a statin were included in this study. Those with a concurrent diagnosis of diseases with elevation of creatine kinase (CK) (U/L) were excluded. The patients were stratified by CK level into mild < 1000, moderate 1000-5000, and severe > 5000. Demographic, clinical, and laboratory data were compared between the CK groups using the Pearson’s Chi-squared test, Fisher’s exact test, and the Kruskal-Wallis rank sum test.
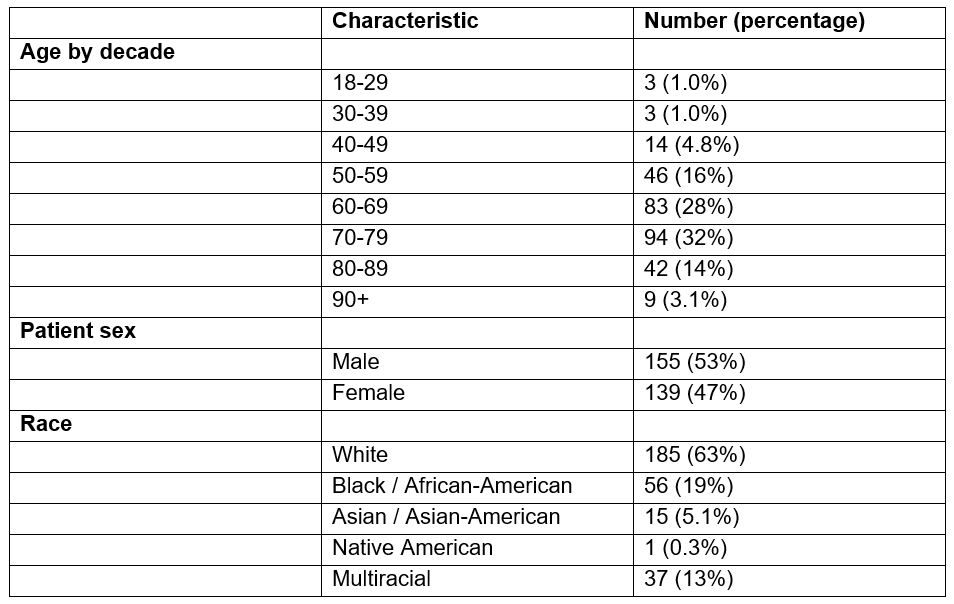
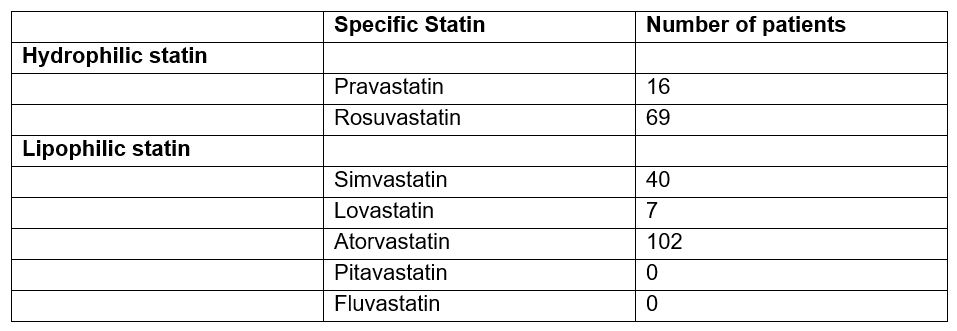
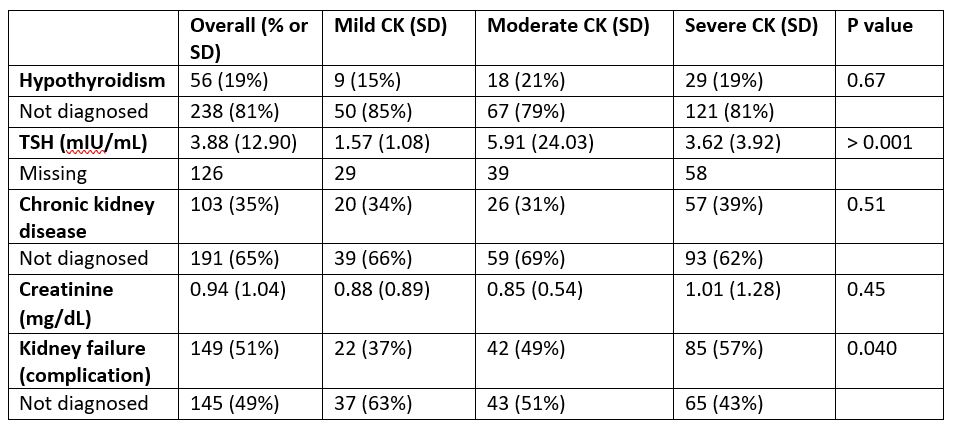
Results: There were 294 subjects. 59 of the patients were in the mild CK group, 85 in the moderate group, and 150 in the severe group. Most of the patients were older, and 47% were female. 63% were white (Table 1). 84 patients were on a hydrophilic statin, and 143 were on a lipophilic statin (Table 2). The daily statin dose amongst the three groups were statistically different (p < 0.001) with higher doses in the severe group; however, the only medication with statistically different doses amongst the CK groups was rosuvastatin (p < 0.001). 25% of the patients had chronic kidney disease. 20% of them had hypothyroidism. The average TSH is 3.88 mIU/mL. The average creatinine was 2.18 mg/dL. 51% of patients developed kidney failure, and this was significant between groups (p = 0.040) (Table 3). No one was diagnosed with disseminated intravascular coagulation or compartment syndrome. 32 were admitted to the ICU. Death occurred in 12 patients.
Conclusion: This study revealed those at higher risk for rhabdomyolysis were unsurprisingly older but more male than expected. 35% of patients have chronic kidney disease, and 51% had kidney failure, but the etiology could not be established from the data available. 19% had hypothyroidism. The TSH levels in the study groups were statistically different. Patients with hypothyroidism on statin are known to have a higher risk of rhabdomyolysis. Although the statins most implicated in rhabdomyolysis are atorvastatin and simvastatin, rosuvastatin was the only one found to be statistically associated with different levels of CK (p < 0.001). More studies should look at renal disease in rhabdomyolysis and characterize the patients admitted to the ICU.
To cite this abstract in AMA style:
Yang O, VENKAT K, Durbin J, Kubomoto S. Characterization of Statin Induced Myopathy in the Hospital Setting [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/characterization-of-statin-induced-myopathy-in-the-hospital-setting/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characterization-of-statin-induced-myopathy-in-the-hospital-setting/