Session Information
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Cervical cancer screening is important for women with systemic lupus erythematosus (SLE) and women prescribed TNF-alpha inhibitors (TNFi), as they have an increased risk of cervical dysplasia and cancer due to immune dysfunction and/or suppression. We describe receipt of guidelines-concordant cervical cancer screening among women receiving rheumatology care in a large Pennsylvania healthcare system. We explored whether women with SLE or prescribed TNFi would be more likely to receive guideline-concordant screening than women with average risk of cervical cancer.
Methods: Cervical cancer screening was compared between women ages 18-50 who had ≥ 2 rheumatology visits between 2007 and 2014, ≥ 1 documented screening test, and diagnosis of SLE or usage of TNFi’s (cases) vs. fibromyalgia only (control). Outcomes and predictors were identified in the electronic health record by medication lists, ICD-9 and procedure codes. Guideline-concordant screening was defined as adherence with contemporaneous U.S. guidelines (Table 1), with six-month buffers added to each testing interval to account for potential scheduling constraints. Descriptive statistics were calculated and compared between groups using Chi-square or two-sample t-tests. Logistic regression was used to evaluate associations between each key predictor and the outcome variable; adjusted models included age, race/ethnicity, health insurance, and documented cervical dysplasia. Women without screening data (SLE: n=108; TNFi: n= 270) were excluded as they may have received screening outside of the healthcare system; however, as some may not have had any screening tests completed, we also performed a separate sensitivity analysis categorizing these women as non-adherent with guidelines.
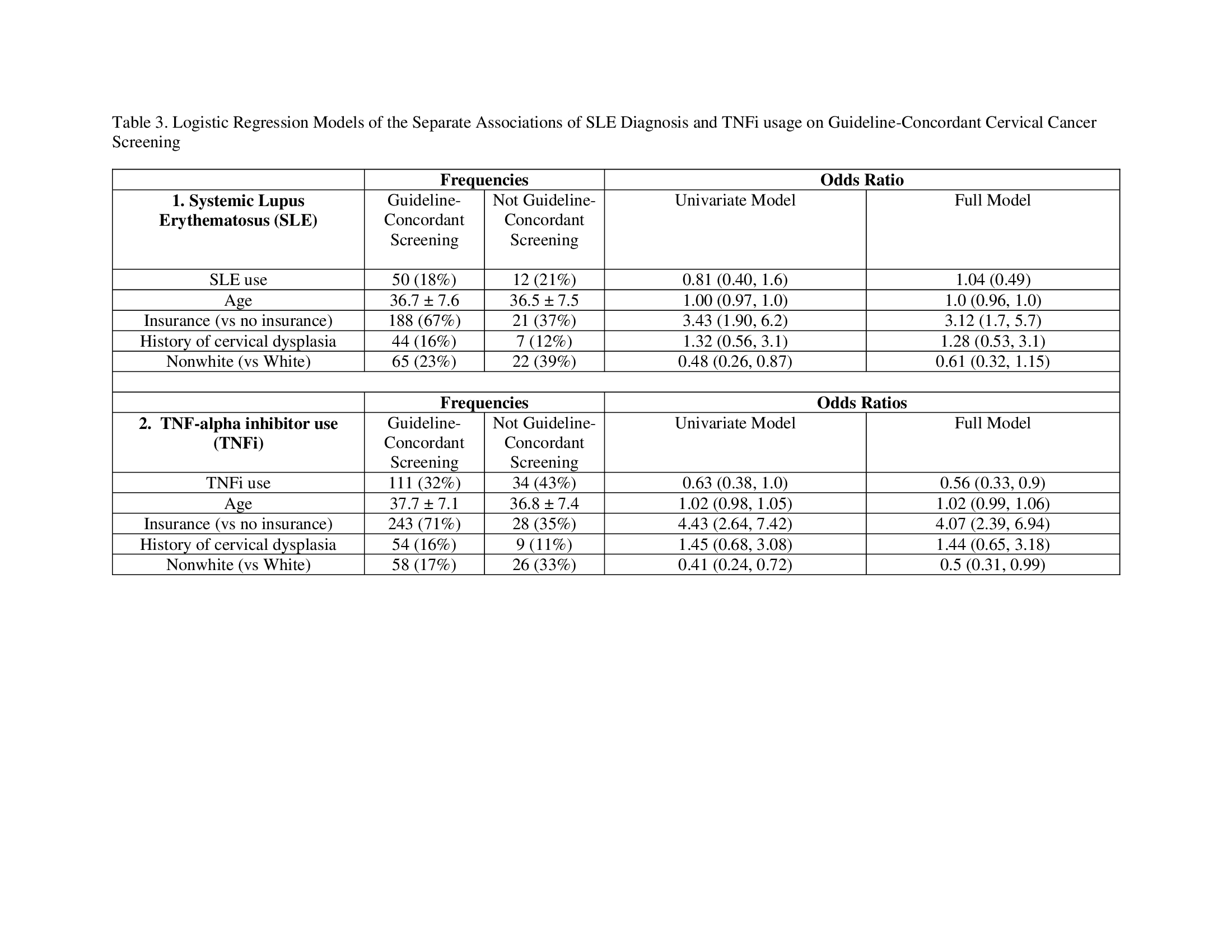
Results: Table 2 describes characteristics of controls (n=867), SLE cases (n=160), and TNFi cases (n=415). Guideline-concordant screening was conducted for 84% for controls, and 81% for SLE and 77% for TNFi cases. SLE cases were as likely as controls to receive guideline-concordant screening (OR 1.04, 95% CI: 0.49, 2.2) (Table 3), whereas TNFi cases were significantly less likely (aOR 0.56, 95% CI: 0.33, 0.95). As compared to whites, guideline-concordant screening was also less likely among non-white TNFi cases (aOR 0.55, 95% CI: 0.31, 0.99) and marginally less likely among non-white SLE cases (aOR 0.61, 95% CI: 0.32, 1.2). Having health insurance was associated with guideline-concordant screening among cases. Primary care or gynecology visits did not explain differences in screening. In sensitivity analyses, the relationship between SLE and guideline-concordant screening was unchanged but was attenuated for TNFi cases.
Conclusion: Women at increased risk of cervical dysplasia/cancer were not more likely to receive guideline-concordant cervical cancer screening than women with average risk, and women who used TNFi were significantly less likely. Rheumatologists should help to ensure that patients with elevated cervical cancer risk are informed about their risks and referred for appropriate screening; additional strategies to ensure screening equity for marginalized populations must also be identified.


To cite this abstract in AMA style:
Birru Talabi M, Jeong K, Abebe K, Clowse M, Domsic R, Borrero S. Cervical Cancer Screening Among Women with Systemic Lupus Erythematosus or Prescribed Tumor Necrosis Alpha-inhibitors Who Receive Outpatient Rheumatology Care [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/cervical-cancer-screening-among-women-with-systemic-lupus-erythematosus-or-prescribed-tumor-necrosis-alpha-inhibitors-who-receive-outpatient-rheumatology-care/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cervical-cancer-screening-among-women-with-systemic-lupus-erythematosus-or-prescribed-tumor-necrosis-alpha-inhibitors-who-receive-outpatient-rheumatology-care/