Session Information
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: This study evaluated the prevalence and
progression of subclinical carotid artery atherosclerosis in active rheumatoid
arthritis (RA).
Methods: Carotid arteries of RA patients were scanned using high
resolution 3D ultrasound at baseline and 24 weeks for vessel wall volume,
intima-media thickness (IMT) and total plaque area, as well as arterial
stiffness measured using pulse wave velocity. Variables related to
inflammation, lipids and cardiovascular risk were assessed for associations
with plaque progression. Of 195 screened patients, 31 met inclusion
criteria (66 Swollen joint count (SJC) plus 68 Tender joint count (TJC)³8 OR
SJC plus TJC³4 with elevated acute phase reactants) and were enrolled (27
female; mean age 59.3±9.8 years). Patients using lipid lowering drugs and
uncontrolled comorbidities were excluded.
Results: Atherosclerotic plaque occurred in 35% and arterial
wall hypertrophy (IMT³0.6mm) in 86% of patients. Most (68%) had an atherogenic
lipid profile characterized by reduced HDL and/or increased total
cholesterol/HDL index, which was adversely affected by disease activity.
Stepwise binary logistic regression analysis showed that Framingham risk score
(OR=1.155, 95%CI:1.002-1.332, p=0.046) and ESR (OR=1.148, 95%CI:1.015-1.299,
p=0.028) predicted plaque most strongly (table). Plaque progression was
significantly associated with baseline higher hsCRP, ESR, and heavy smoking,
but only hsCRP predicted plaque growth in multivariate regression analysis
(p=0.004); and hsCRP was related to higher disease activity (r=0.443, p=0.016),
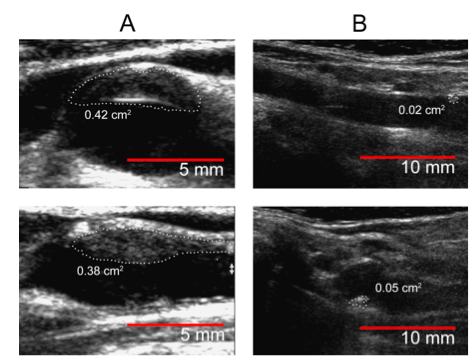
LDL (r=0.544, p=0.007), and smoking (r=0.384, p=0.04). Figure shows
carotid artery plaque with and without progression.
Conclusion:
RA-related
inflammation contributed to augmented CV burden in RA and might mediate its
effect on atherosclerosis through hsCRP and modulation of the traditional CV
risk factors, such as dyslipidemia.
|
RA patients with plaque, n = 11
|
RA patients without plaque, n = 20
|
P-value
|
|
|
Clinical characteristics |
|||
|
Age, years (SE) |
63.2 (8.9) |
57.1 (9.8) |
0.1 |
|
Disease duration, years
|
18.1 (12.0) |
13.8 (9.5) |
0.29 |
|
DAS 28-ESR (SE) |
4.9 (1.1) |
4.8 (1.3) |
0.81 |
|
DAS 28-CRP (SE) |
4.5 (1.2) |
4.6 (1.2) |
0.86 |
|
Hypertension, n (%) |
7 (64) |
10 (50) |
0.46 |
|
Body mass index (SE) |
27.6 (7.8) |
30.6 (5.8) |
0.36 |
|
Smoking history: Current smokers, n (%) Former smokers, n (%) Never smokers, n (%) |
9(36) 4 (36) 3 (28) |
6(30) 7(35) 7 (35) |
0.53 |
|
Family history of cardiovascular disease, n (%) |
5 (46) |
5 (25) |
0.24 |
|
Framingham risk score |
19.2 (12.1) |
10.5 (6.6) |
0.005
|
|
Creatinine clearance (Cockcroft-Gault equation) |
0.93 (0.36) |
1.16 (0.19) |
0.002 |
|
ESR, mm/hr (SE) |
30.2 (14.2) |
17.7 (15.4) |
0.009 |
|
hsCRP, mg/l (SE)
|
9.5 (7.7) |
6.7 (6.5) |
0.33 |
|
Total cholesterol, mmol/l (SE) |
4.9 (0.8) |
5.1 (0.8) |
0.64 |
|
LDL cholesterol, mmol/l (SE) |
2.9 (0.6) |
3.0 (0.7) |
0.42 |
|
HDL cholesterol, mmol/l (SE) |
1.52 (0.5) |
1.4 (0.5) |
0.52 |
|
Total/HDL cholesterol (AI) (SE) |
3.6 (1.5) |
4.1 (1.5) |
0.42 |
Figure. Baseline
3D ultrasound measures of total plaque area (TPA) in two patients with
rheumatoid arthritis indicative of atherosclerotic plaque occurrence (patient
A; TPA -0.8mm2) and normal carotid artery wall (patient B. TPA –
0.07mm2). The cross-sectional area of each plaque was measured in
the longitudinal view. TPA was the sum of all plaques between the clavicle and
the angle of the jaw in both left and right carotid
arteries.
To cite this abstract in AMA style:
Nevskaya T, Pope JE, Barra L, Parraga G. Carotid Artery Atherosclerosis in Patients with Active Rheumatoid Arthritis: Predictors of Plaque Occurrence and Progression over 24 Weeks [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/carotid-artery-atherosclerosis-in-patients-with-active-rheumatoid-arthritis-predictors-of-plaque-occurrence-and-progression-over-24-weeks/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/carotid-artery-atherosclerosis-in-patients-with-active-rheumatoid-arthritis-predictors-of-plaque-occurrence-and-progression-over-24-weeks/