Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Romosozumab (romo) and denosumab (dmab) are recommended for postmenopausal women with osteoporosis (OP) at high risk of fracture. The U.S. prescribing information includes a boxed warning that romo should not be initiated in patients with prior myocardial infarction or stroke in the prior year. Forall other patients without recent MI or stroke, the warning recommends to consider whether the benefits of romo outweigh its risks. This study evaluated CV and fracture risks among patients who initiated romo referent to dmab users.
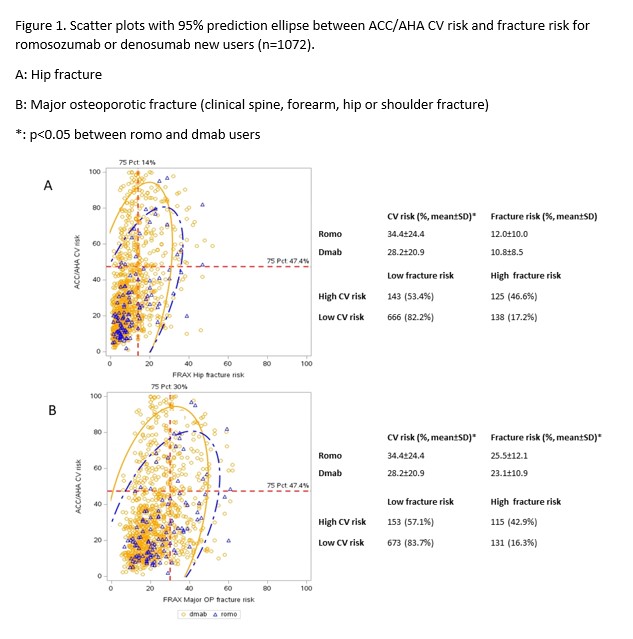
Methods: We used Medicare data from 1/1/2017 to 9/30/2021 to identify women age ≥55 newly initiating romo or dmab after 4/1/2019.Claims data was linked to electronic medical record (EMR) data from multiple PCORNet Clinical Research Networks. Comorbidities and medical history were identified from claims while biometric data and lipid test results were obtained from the EMR. The ACC/AHA pooled cohort risk equation was used to calculate the 10-year CV risk. The FRAX algorithm was used to calculate 10-year risk of hip and major fracture (clinical spine, forearm, hip, or shoulder). We set the 75 percentile of each risk score as the cut-off for high CV and fracture risk. A scatter plot with 95% prediction ellipse was used to illustrate the relationship between CV risk versus the risk of fractures (Figure 1) at a patient level and to compare the cohort of romo vs. dmab patients. Multivariable logistic regression was used to evaluate the relationship between high CV or fracture risk and medication initiation.
Results: A total of 197,515 new users of romo(n=14,596)or dmab (n=182,919) were eligible for analysis and 1072 were linked to PCORNet data. Figure 1 showed romo users had lower CV risk but comparable or higher risk for hip or major fracture compared with dmab users. Romo was more likely to be prescribed to patients with higher fracture risk but lower CV risk, compared with dmab. The odds ratios (95% CI) for initiating romo vs. dmab for high CV risk, hip fracture risk, and major fracture risk were 0.46 (0.26, 0.80), 0.97 (0.47, 2.01), and 1.83 (0.89, 3.75), respectively.
Conclusion: In this cohort of older women with claims data linked to EHR data, patients with high CV risk were less likely to be given romo compared with dmab. These data suggest that the boxed warning regarding CV risk for romo appropriately influences clinical decision making of physicians when prescribing anabolic medications for osteoporosis patients.
To cite this abstract in AMA style:
Liu Y, Arora T, Tanner S, Curtis J. Cardiovascular Risk and Fracture Risk Among Women Initiating Treatment with Romosozumab or Denosumab [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/cardiovascular-risk-and-fracture-risk-among-women-initiating-treatment-with-romosozumab-or-denosumab/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cardiovascular-risk-and-fracture-risk-among-women-initiating-treatment-with-romosozumab-or-denosumab/