Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: The relationship between juvenile spondyloarthritis (JSpA) and chronic nonbacterial osteomyelitis (CNO) remains poorly defined. This study aimed to assess the proportion of pediatric patients who meet classification criteria for both JSpA and CNO, characterize the clinical and radiologic overlap between the two conditions, and compare initial treatment approaches within the first 6 months following diagnosis.
Methods: This was a retrospective cohort study conducted on children (≤18 years) diagnosed with JSpA and CNO between 2016 and 2024 at a tertiary care children’s hospital. Subjects were identified by electronic health record coding and included if they had: at least 2 rheumatology visits, no prior biologic therapy, and met at least one set of classification criteria: ILAR PsA/ERA or European Spondyloarthropathy Study Group (ESSG) (for JSpA), or Bristol or Jansson (for CNO). Overlap was defined as present if at least one set of JSpA and CNO criteria were met. The index visit was defined as the first clinical encounter with a JSpA or CNO diagnostic code. Data from the 6 months following the index visit – including demographics, clinical symptoms, family history, lab values, and imaging – were abstracted into a REDCap database. Descriptive statistics were calculated using medians and interquartile ranges (IQR) and proportions. Between-group comparisons were conducted using Mann-Whitney U and Chi-square tests, as appropriate.
Results: A total of 137 subjects met inclusion criteria. Of these, 20 (14.6%) met criteria for both JSpA and CNO. This overlap group was significantly older (p< 0.001) and predominantly female (75.0%) (Table 1). Psoriasis was observed significantly more frequently in the overlap group compared to JSpA or CNO alone (55%, 20.8%, 3.1%, respectively; p< 0.001). In contrast, peripheral arthritis and enthesitis were significantly less common in the CNO cohort (both p< 0.001). Whole-body/pelvic MRI were obtained in 13.2%/50.9% of JSpA, 89.1%/25.0% of CNO, and 30.0%/30.0% of overlap patients, respectively. Figure 1 shows the distribution of the most frequently involved sites of disease activity across the 3 groups. Pelvic osteitis and/or sacroiliitis affected approximately one-third of cases across all groups, with sacroiliitis significantly more common in JSpA (p=0.003). NSAIDs and TNF inhibitors were the most frequently prescribed therapies in all 3 groups (Figure 2). DMARDs were used more often in the JSpA and overlap groups, while bisphosphonates were more commonly prescribed for CNO. The most commonly met criteria in each diagnosis was ESSG criteria (66.0%) for JSpA patients, Bristol criteria (85.9%) for CNO patients, and ESSG (70.0%) and Jansson (70.0%) for overlap patients.
Conclusion: A subset of pediatric patients fulfilled classification criteria for both JSpA and CNO, with overlapping clinical and radiologic features. The co-occurrence of these conditions may represent a distinct phenotype, characterized by older age, female predominance, and a higher prevalence of psoriasis. Differences in imaging use and treatment strategies highlight the importance of recognizing this overlap for appropriate diagnostic clarity, evaluation and therapeutic decision-making.
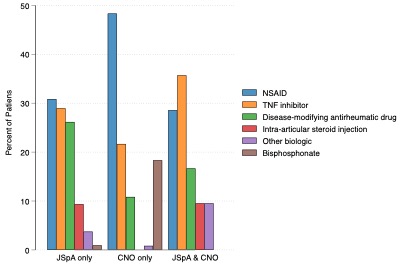 Table 1. Demographic and clinical information about study cohort (n=137). ^HLA-B27 status unavailable on 4 JSpA patients, 43 CNO patients, and 5 JSpA/CNO patients.
Table 1. Demographic and clinical information about study cohort (n=137). ^HLA-B27 status unavailable on 4 JSpA patients, 43 CNO patients, and 5 JSpA/CNO patients.
.jpg) Figure 1. Sites of active disease were identified through clinical examination and/or imaging. Statistically significant values (p < 0.05) are highlighted in blue and red.
Figure 1. Sites of active disease were identified through clinical examination and/or imaging. Statistically significant values (p < 0.05) are highlighted in blue and red.
.jpg) Figure 2. Treatments prescribed in the first six months after the index visit.
Figure 2. Treatments prescribed in the first six months after the index visit.
To cite this abstract in AMA style:
Elfrink S, Brandon T, Jazayeri J, Weiss P. Bridging the Gap: Juvenile Spondyloarthritis (JSpA) vs. Chronic Non-Bacterial Osteomyelitis (CNO) [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/bridging-the-gap-juvenile-spondyloarthritis-jspa-vs-chronic-non-bacterial-osteomyelitis-cno/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bridging-the-gap-juvenile-spondyloarthritis-jspa-vs-chronic-non-bacterial-osteomyelitis-cno/