Session Information
Date: Sunday, November 12, 2023
Title: (0510–0542) Spondyloarthritis Including Psoriatic Arthritis – Treatment: AxSpA Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Pain and fatigue have been identified by patients (pts) as key features of PsA, driving the impact on their health-related quality of life.1 Bimekizumab (BKZ), a monoclonal IgG1 antibody that selectively inhibits IL-17F in addition to IL-17A, has demonstrated meaningful improvements in pain and fatigue outcomes to 16 weeks (wks) vs placebo (PBO) in pts with active PsA.2,3 In this study, pt-reported pain and fatigue outcomes are reported up to 1 year from two phase 3 studies of BKZ in pts with PsA.
Methods: BE OPTIMAL (NCT03895203) and BE COMPLETE (NCT03896581) were two phase 3 trials assessing BKZ in pts with active PsA who were biologic DMARD (bDMARD)-naïve or had inadequate response or intolerance to 1–2 TNF-α inhibitors (TNFi-IR), respectively. Both trials had a 16-wk double-blind, PBO-controlled phase.
Pts in BE OPTIMAL were randomized 3:2:1 to subcutaneous (sc) BKZ 160 mg every 4 wks (Q4W), PBO, or reference (sc adalimumab [ADA] 40 mg Q2W). At Wk 16, PBO pts switched to receive BKZ until Wk 52 (PBO/BKZ); pts receiving BKZ or ADA continued their dosing until Wk 52. BE OPTIMAL ADA data are not reported here. Pts in BE COMPLETE were randomized 2:1 to sc BKZ 160 mg Q4W or PBO. Along with BE OPTIMAL Wk 52 completers, pts who completed Wk 16 of BE COMPLETE were eligible to enter an open-label extension, BE VITAL (NCT04009499); PBO pts switched to BKZ (PBO/BKZ) on entry (36 wks of BKZ treatment to Wk 52); BE COMPLETE plus BE VITAL is referred to as ‘BE COMPLETE’ hereafter.
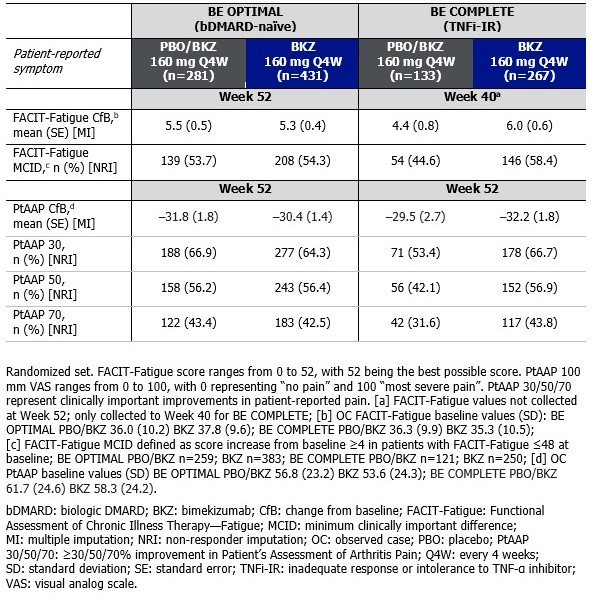
Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-Fatigue) subscale Minimum Clinically Important Difference (MCID; ≥4-point improvement from baseline [BL]) and change from BL (CfB), along with Pt’s Assessment of Arthritis Pain (PtAAP) CfB and clinically important improvements (≥30/50/70%), are reported up to 1 year. BE COMPLETE FACIT‑Fatigue values were collected to Wk 40 only. Non-responder and multiple imputation (NRI, MI) were used for missing binary and continuous variables.
Results: Overall, 770/852 (90.4%) and 347/400 (86.8%) pts completed Wk 52 of BE OPTIMAL and BE COMPLETE, respectively.
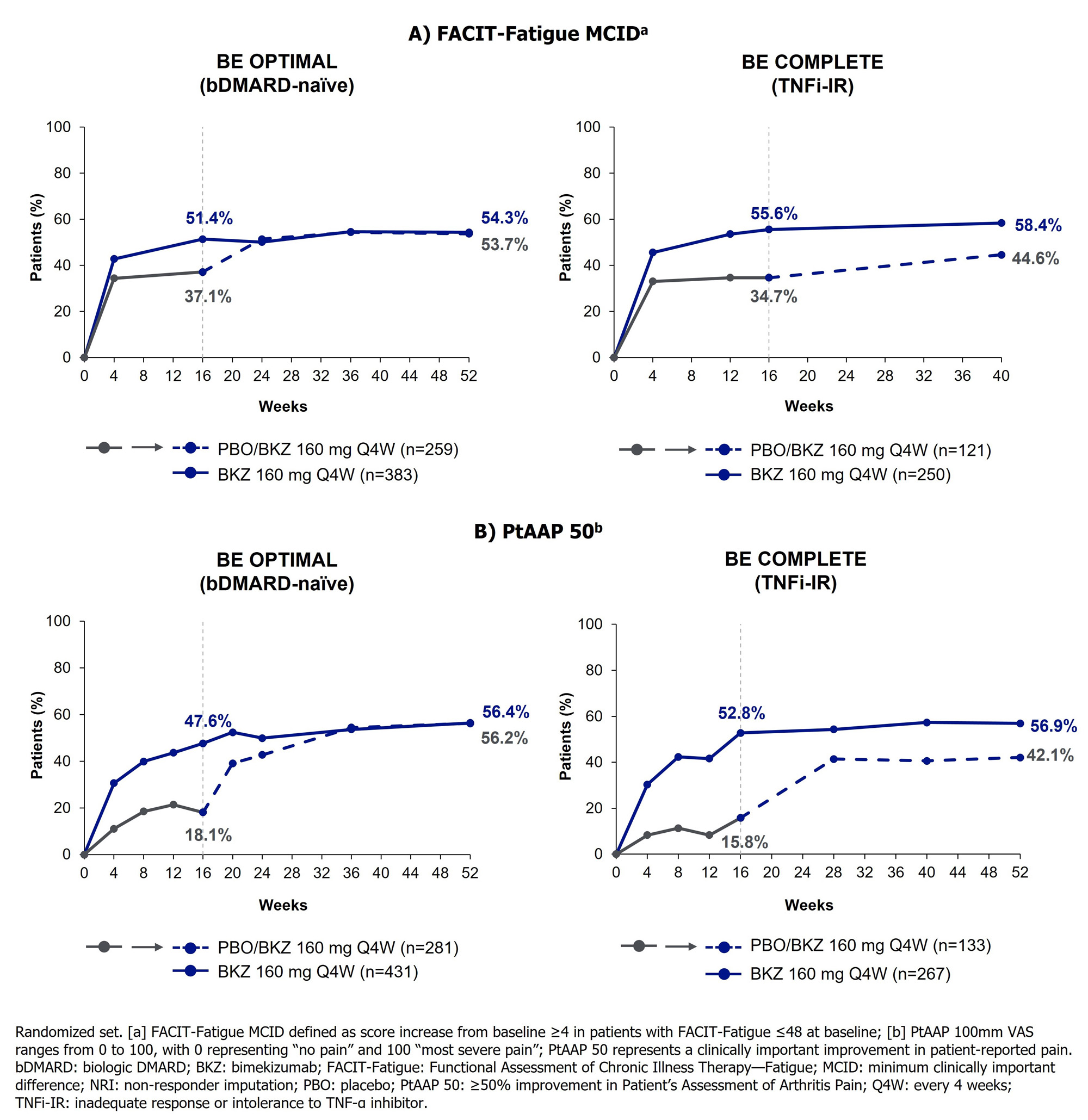
At Wk 16, BKZ-treated pts achieved greater improvements in pain and fatigue outcomes vs PBO pts (Figure); improvements were sustained from Wk 16 to Wk 52 on BKZ treatment. For PBO/BKZ pts, pain and fatigue outcomes improved following switch to BKZ (Table).
Of pts with FACIT-Fatigue ≤48 at BL, FACIT-Fatigue MCID was achieved by 208/383 (54.3%) BKZ and 139/259 (53.7%) PBO/BKZ pts at Wk 52 in BE OPTIMAL, and 146/250 (58.4%) BKZ and 54/121 (44.6%) PBO/BKZ pts at Wk 40 in BE COMPLETE (Table, Figure). At Wk 52, PtAAP 50 was achieved by 243/431 (56.4%) BKZ and 158/281 (56.2%) PBO/BKZ pts in BE OPTIMAL, and 152/267 (56.9%) BKZ and 56/133 (42.1%) PBO/BKZ pts in BE COMPLETE.
Conclusion: Treatment with BKZ resulted in sustained improvements in pt‑reported pain and fatigue from Wk 16 up to 1 year in both bDMARD-naïve and TNFi-IR pts with active PsA, with clinically meaningful improvements observed in over half of pts. Improvements in pt‑reported pain and fatigue were similar between the two studies, demonstrating consistent responses in bDMARD-naïve and TNFi-IR pts.
References:1. Ogdie A. RMD Open 2020;6:e001321;2. McInnes IB. Lancet 2023;401:25–37; 3. Merola JF. Lancet 2023;401:38–48.
To cite this abstract in AMA style:
Husni M, Mease P, Merola J, Behrens F, Favalli E, McGonagle D, Tillett W, Tsuji S, Ink B, Bajracharya R, Lambert J, Coarse J, Gossec L. Bimekizumab Treatment Impact on Pain and Fatigue in Patients with Active Psoriatic Arthritis Who Were Biologic DMARD‑Naïve or Had Inadequate Response or Intolerance to TNF-α Inhibitors: 1-Year Results from Two Phase 3 Studies [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/bimekizumab-treatment-impact-on-pain-and-fatigue-in-patients-with-active-psoriatic-arthritis-who-were-biologic-dmard%e2%80%91naive-or-had-inadequate-response-or-intolerance-to-tnf-%ce%b1-inhibitors-1/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bimekizumab-treatment-impact-on-pain-and-fatigue-in-patients-with-active-psoriatic-arthritis-who-were-biologic-dmard%e2%80%91naive-or-had-inadequate-response-or-intolerance-to-tnf-%ce%b1-inhibitors-1/