Session Information
Date: Sunday, November 12, 2023
Title: (0380–0422) RA – Diagnosis, Manifestations, and Outcomes Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Quantitative computed tomography (QCT) methods have been developed to automatically quantify parenchymal lung features on chest CT imaging. There have been limited investigations of QCT in RA participants and non-RA comparators or studies of the mortality impact of QCT features in RA. We hypothesized that RA would be associated with increased interstitial changes and emphysema, as determined by QCT. We also hypothesized that QCT scoring of interstitial and emphysematous lung changes would identify RA patients at higher mortality risk.
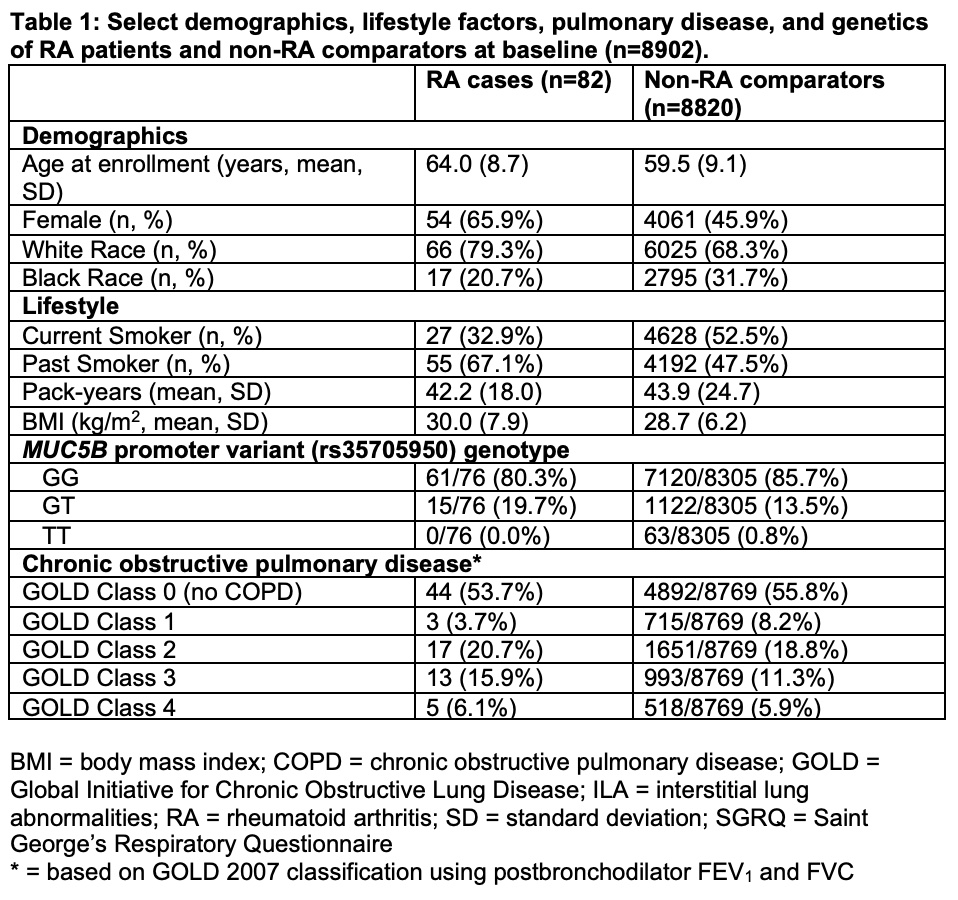
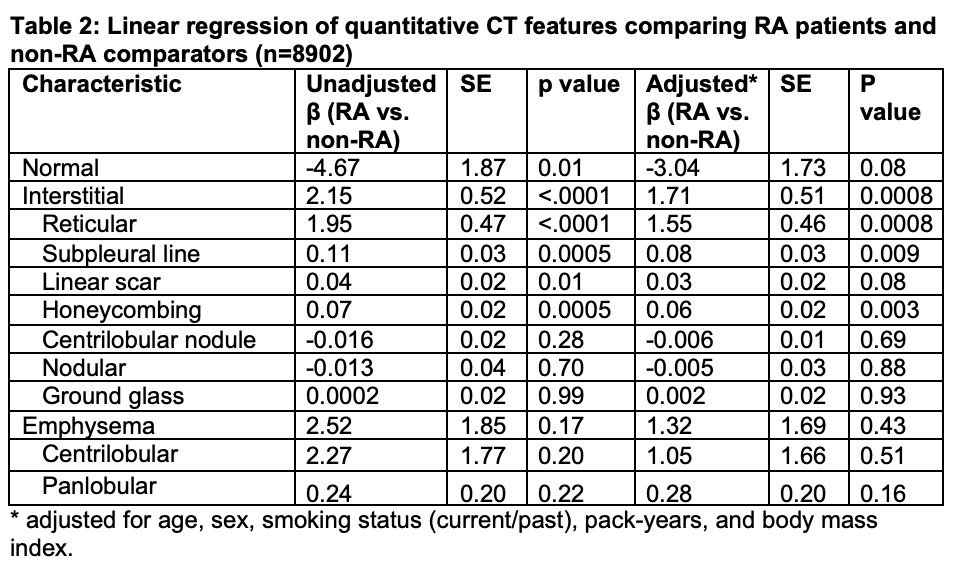
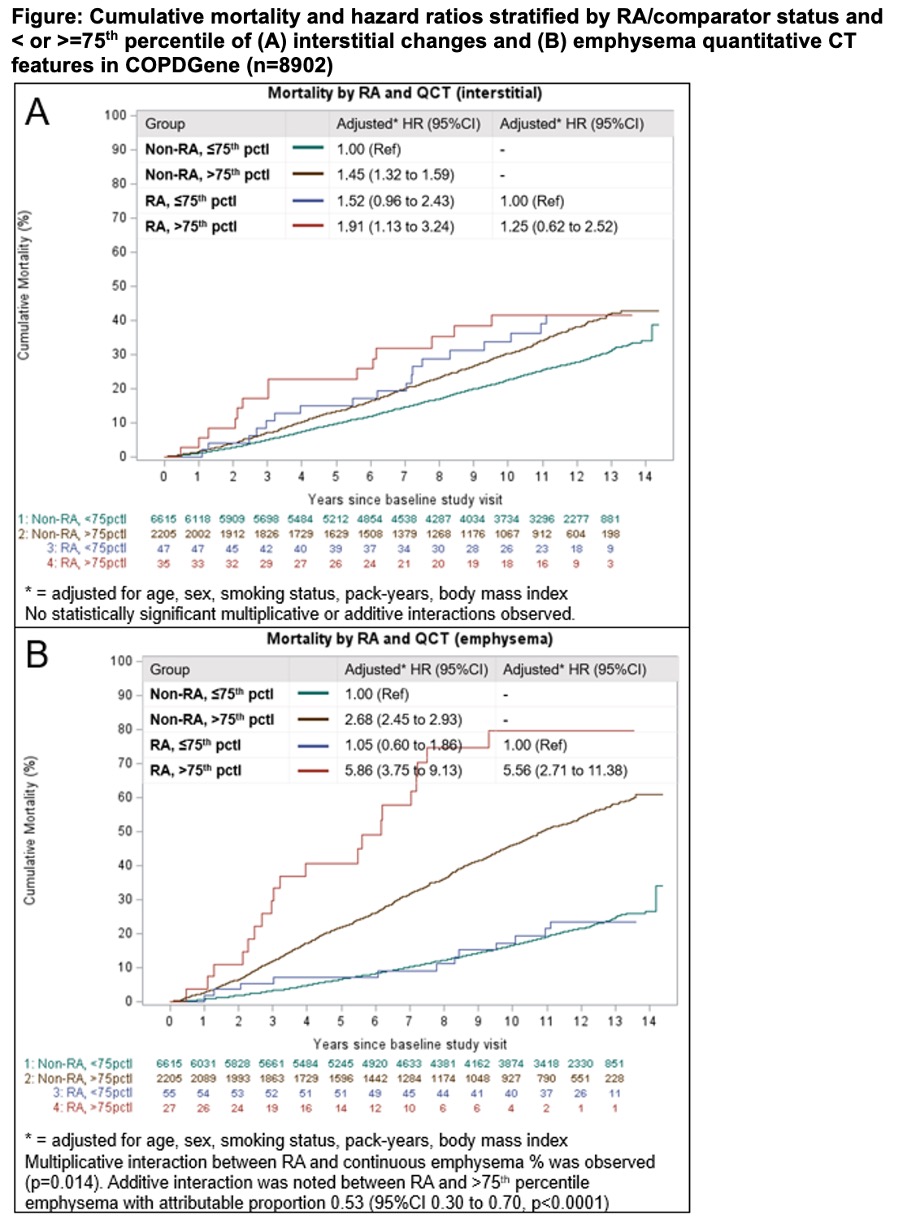
Methods: We investigated associations between RA and QCT features in COPDGene, a multicenter cohort study of current or former smokers that excluded participants with known interstitial lung disease or bronchiectasis. We identified participants with and without RA using RA self-report and DMARD use. We assessed the lung parenchyma in each scan using a k-nearest neighbors classifier that categorizes regions of interest into normal lung, interstitial changes, or emphysema using the local tissue density and distance from the pleural surface. Interstitial changes were subclassified into reticular, subpleural line, linear scar, honeycombing, centrilobular nodule, nodular, and ground glass. Each feature was summed and standardized to total lung volume. We examined associations between QCT features and RA using multivariable linear regression. We dichotomized participants using the 75th percentile for each QCT feature among non-RA participants and investigated mortality associations by RA status and QCT features using Cox regression. We examined multiplicative interactions between RA and continuous interstitial and emphysema percentages and additive interactions between RA status and >75th percentile of QCT features and mortality.
Results: We analyzed 82 RA cases and 8820 non-RA comparators. RA was associated with a lower percentage of normal lung (85.8% vs. 91.0% p=0.0001), increased interstitial changes (7.0% vs. 4.8%, p< 0.0001) and no statistically significant difference in emphysema (2.6% vs. 1.9%, p=0.09) compared to non-RA comparators. In linear regression analyses adjusted for age, sex, smoking status, pack-years, and body mass index, RA was associated with increased interstitial changes (β=1.7±0.5, p=0.0008) but not emphysema (β=1.3±1.7, p=0.44). The combination of RA and >75th percentile of emphysema had significantly higher mortality compared to both non-RA participants (HR 5.86, 95%CI 3.75-9.13) and RA participants (HR 5.56, 95%CI 2.71-11.38) with < 75th percentile of emphysema. There were statistically significant interactions between RA and emphysema for mortality (multiplicative: p=0.014; additive: attributable proportion 0.53, 95%CI 0.30-0.70, p< 0.0001).
Conclusion: Using machine learning-derived QCT data in a cohort of smokers, we found that RA was associated with increased interstitial changes, even after adjustment for smoking and other lifestyle factors. The combination of RA and emphysema conferred greater than 5-fold increased mortality.
To cite this abstract in AMA style:
McDermott G, Hayashi K, Moll M, Cho M, Yoshida K, Doyle T, Kinney G, Dellaripa P, Wallace Z, Regan E, Hunninghake G, Silverman E, Ash S, San Jose Estepar R, Washko G, Sparks J. Associations and Mortality Impact of Machine Learning-derived Quantitative Computed Tomography Parenchymal Lung Features in Rheumatoid Arthritis and non-RA Comparators in a Multicenter Prospective Cohort of Smokers [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/associations-and-mortality-impact-of-machine-learning-derived-quantitative-computed-tomography-parenchymal-lung-features-in-rheumatoid-arthritis-and-non-ra-comparators-in-a-multicenter-prospective-coh/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/associations-and-mortality-impact-of-machine-learning-derived-quantitative-computed-tomography-parenchymal-lung-features-in-rheumatoid-arthritis-and-non-ra-comparators-in-a-multicenter-prospective-coh/