Session Information
Date: Saturday, November 16, 2024
Title: SpA Including PsA – Diagnosis, Manifestations, & Outcomes Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Kinesiophobia, defined as the fear of movement, poses a significant barrier to effective rehabilitation, functional recovery, and adequate physical activity.
To investigate the impact of kinesiophobia on patients with axial spondylo-arthritis (axSpA), and its relation to global functioning and health, disease activity, function, spinal mobility and physical activity in comparison to healthy controls (HC).
Methods: Post-hoc analysis of an observational study in which consecutive patients with axSpA (n=100) and 20 healthy controls (HC) were examined by the Tampa scale of kinesiophobia (TSK), and the Fear avoidance belief questionnaire (FABQ). Patient reported outcomes and objective assessments of disease activity (ASDAS, BASDAI), physical function (BASFI), global health and functioning (ASAS HI), daily level of physical activity (mSQUASH) as well as the BASMI, the AS physical performance index (ASPI) and the Short Physical Performance Battery (SPPB) were collected. Categorical analysis to differentiate results of patients with minimal/low (TSK ≤ 28) and moderate/high (TSK >28) kinesiophobia as well as linear correlations comparing TSK and FABQ with demographic data and clinical assessments were performed.
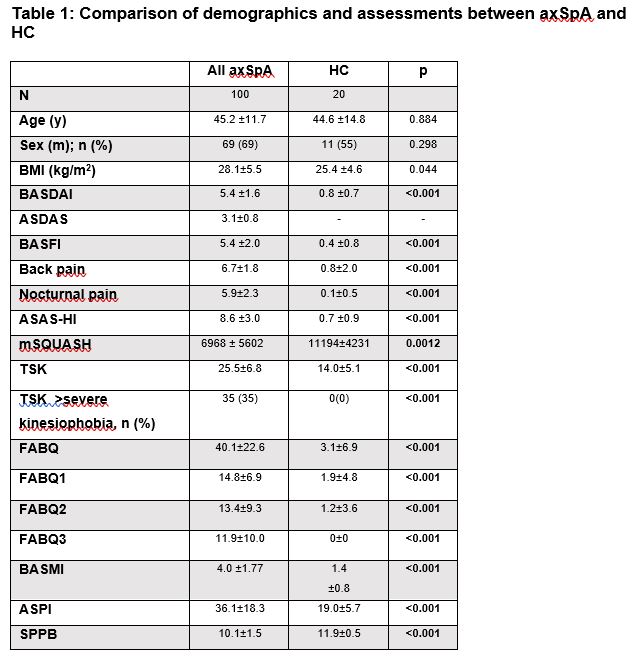
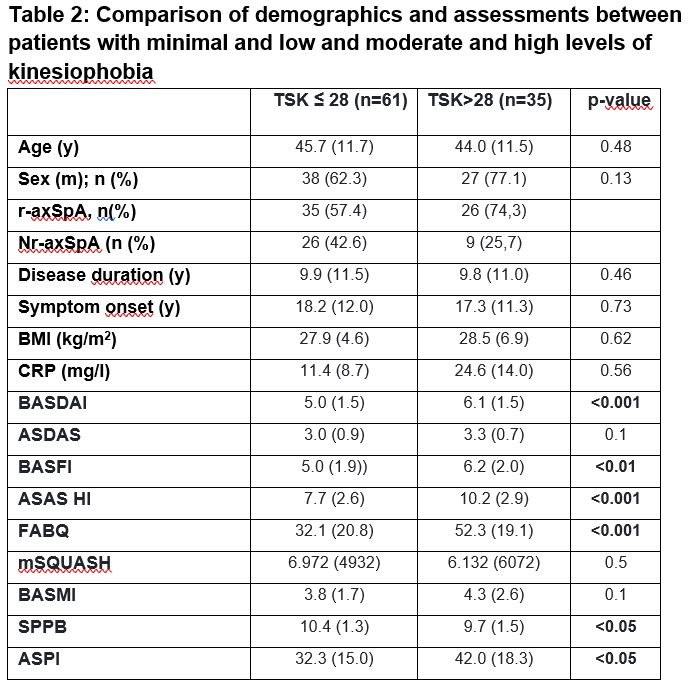
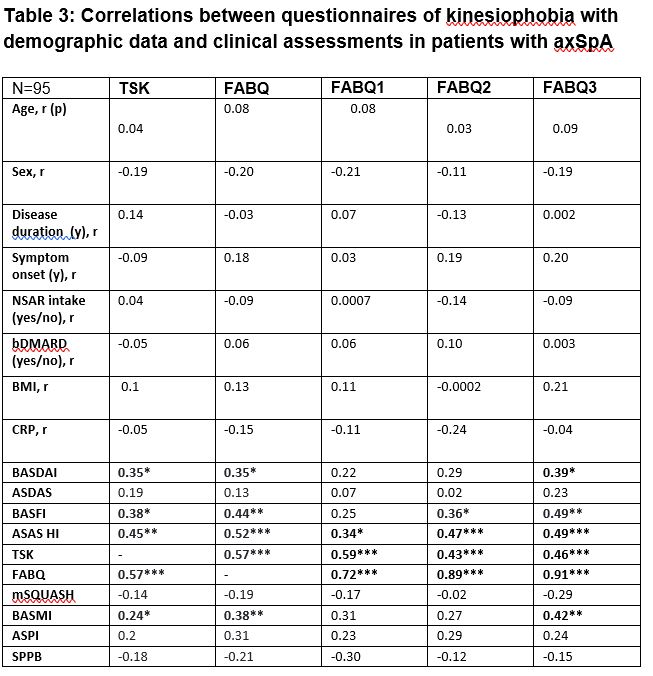
Results: While demographic data for age, sex and BMI were comparable, patients with axSpA showed higher TSK (25.5±6.8 vs 14.0±5.1) and FABQ scores (40.1±22.6 vs 3.1±6.9), worse results for pain, daily level of physical activity (p=0.001) and performance based tests compared to HC, all p≤ 0.001 (Table 1). Categorical analysis of kinesiophobia levels revealed that patients with moderate to high kinesiophobia performed significantly worse in ASPI (32.2±15.0 vs 42.0±18.3) and SPPB (10.4±1.3 vs 9.7±1.5), and showed numerical impairments in BASMI (3.8±1.7 vs 4.3±2.6), (Table 2). Significant correlations between TSK/FABQ and assessments were observed for ASAS HI (r=0.45 and r=0.52) and BASFI (r=0.38 and r=0.44), but not for ASPI, SPPB, mSQUASH. Weak correlations were found for BASMI (r=0.24 and r=0.38) and BASDAI scores (both r=0.35), see Table 3.
Conclusion: Kinesiophobia is a clinically relevant issue for patients with axSpA, with impaired mobility found in patients reporting moderate to high TSK and FABQ scores. The degree of kinesiophobia showed stronger correlations with physical function, global functioning and health than with mobility and physical activity.
To cite this abstract in AMA style:
Kiefer D, Braun J, Kiltz U, Kolle N, Schneider L, Andreica I, Buehring B, Sewerin P, Redeker I, Tsiami S, Herbold S, Baraliakos X. Associations and Impact of Kinesiophobia on Patient Reported Outcomes and Performance-based Mobility Measures in Patients with Axial Spondyloarthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/associations-and-impact-of-kinesiophobia-on-patient-reported-outcomes-and-performance-based-mobility-measures-in-patients-with-axial-spondyloarthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/associations-and-impact-of-kinesiophobia-on-patient-reported-outcomes-and-performance-based-mobility-measures-in-patients-with-axial-spondyloarthritis/