Session Information
Date: Tuesday, November 12, 2019
Title: RA – Diagnosis, Manifestations, & Outcomes Poster III: Comorbidities
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Pulmonary involvement in rheumatoid arthritis (RA), such as bronchiectasis, bronchiolitis, pleuritis, or interstitial lung disease (ILD), is associated with high morbidity and mortality. Pulmonary function testing (PFT) assesses for a wide range of pulmonary abnormalities, broadly characterized as restrictive or obstructive. Seropositive RA patients may be more likely to have restriction, commonly present in ILD. Obstruction may also be more common in seropositive RA related to smoking and airway mucosa as a possible initiating site for RA-related autoantibody development. Therefore, we aimed to determine whether RA-related autoantibodies were associated with abnormalities on PFTs.
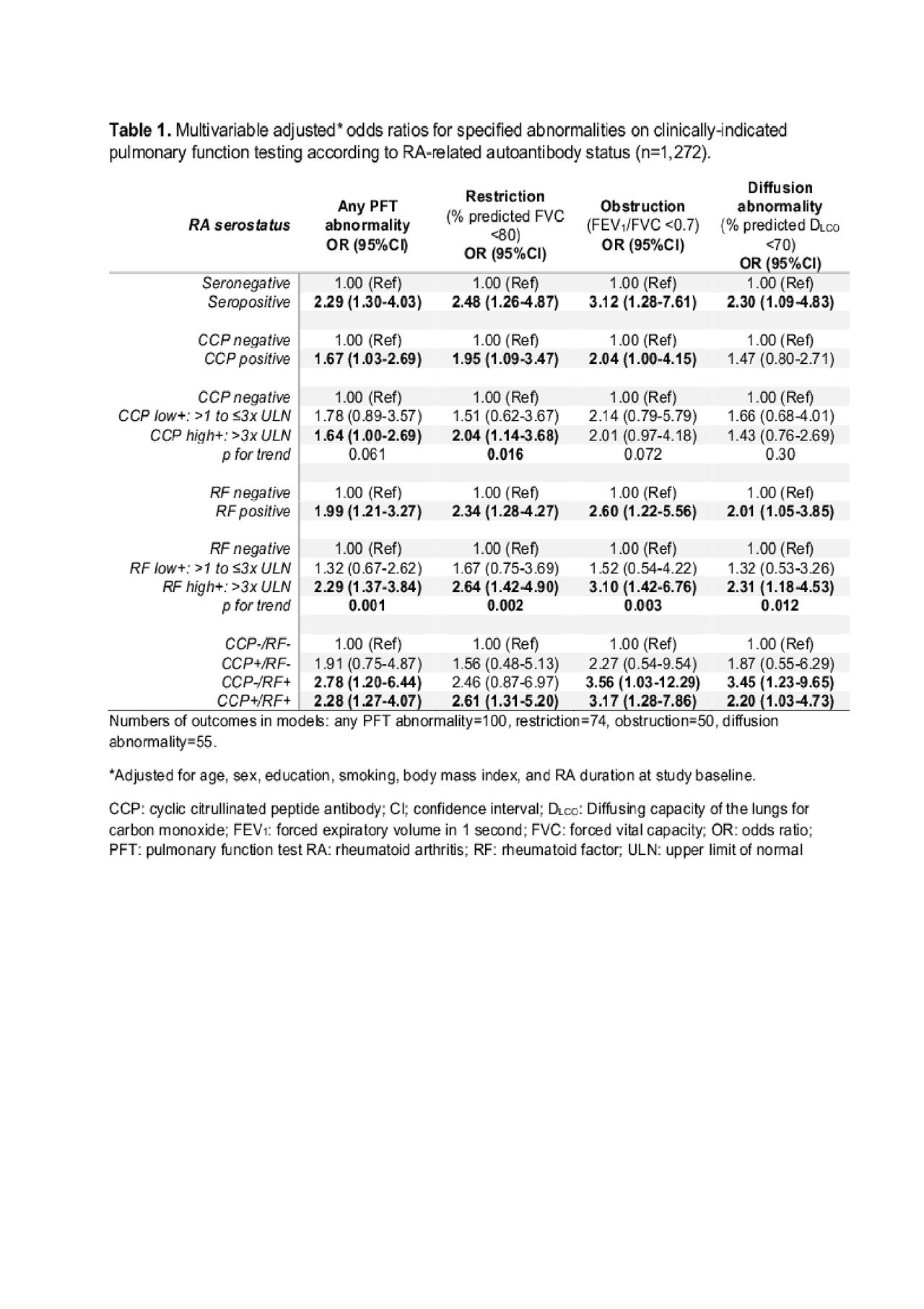
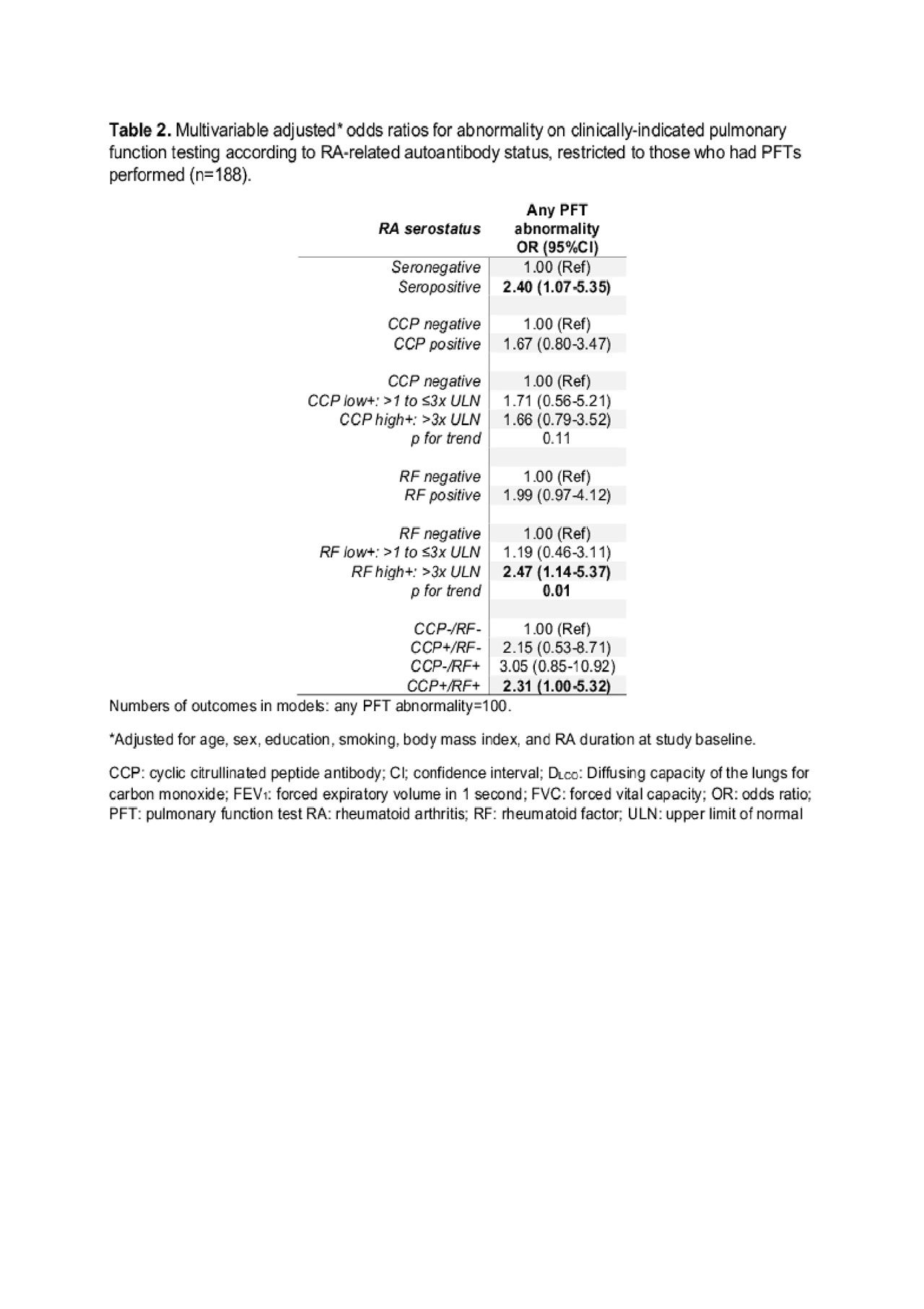
Methods: We investigated RA serostatus and PFT abnormalities using a single center prospective RA registry. RA serostatus was assessed by commercial assays for cyclic citrullinated peptide (CCP) and rheumatoid factor (RF) obtained at baseline for research purposes. We used standard cutpoints to define presence and level of positivity for each autoantibody. Outcomes were abnormalities on clinically-indicated PFTs: restriction (% predicted forced vital capacity [FVC] < 80), obstruction (ratio of forced expiratory volume in one second to FVC [FEV1/FVC] < 0.7), diffusion abnormality (% predicted diffusing capacity of the lungs for carbon monoxide [DLCO] < 70), and a composite of any abnormality. Logistic regression estimated ORs and 95%CIs for types of PFT abnormalities by RA-related autoantibody status, adjusted for possible confounders. We also analyzed only those who had PFTs performed.
Results: Among 1,272 analyzed subjects, mean age was 56.3 years (SD 14.1), 82.2% were female, 69.5% were seropositive (CCP+ or RF+), and 6.8% had ILD. There were 100 subjects with abnormal PFTs. Seropositivity was associated with increased odds of any PFT abnormality (multivariable OR 2.29, 95%CI 1.30-4.03, Table 1) compared to seronegativity. When analyzing by type of PFT abnormality, seropositivity was associated with restriction, obstruction, and diffusion abnormality; multivariable ORs were 2.48 (95%CI 1.26-4.87), 3.12 (95%CI 1.28-7.61), and 2.30 (95%CI 1.09-4.83), respectively. When analyzing by CCP and RF status, the associations were stronger for RF+ than for CCP+ (any PFT abnormality: OR 1.99, 95%CI 1.21-3.27 for RF+ vs. RF-; OR 1.67, 95%CI 1.03-2.69 for CCP+ vs. CCP-), with a dose effect of higher RF levels increasing odds for each PFT abnormality (p for trend< 0.05). Results were similar when only analyzing subjects who had PFTs performed (seropositivity: OR 2.40 (95%CI 1.07-5.35 vs. seronegativity, Table 2).
Conclusion: Seropositive RA patients had 2-fold increased risk for abnormalities on PFTs performed for clinical indications compared to seronegative RA. This association was present for all types of PFT abnormalities and was not explained by smoking. Patients with seropositivity may be at risk for obstructive lung diseases, in addition to the previously known association of seropositivity with restrictive lung diseases, such as ILD. Future studies should assess the value of screening for PFT abnormalities in seropositive RA patients, particularly those with high-titer RF+.
Serostatus and PFTs-ACR abstract-tab1
Serostatus and PFTs-ACR abstract-tab2
To cite this abstract in AMA style:
Huang S, He X, Doyle T, Zaccardelli A, Marshall A, Friedlander H, Blaustein R, Smith E, Iannaccone C, Mahmoud T, Weinblatt M, Dellaripa P, Shadick N, Sparks J. Association of Rheumatoid Arthritis-related Autoantibodies with Pulmonary Function Test Abnormalities in a Prospective Rheumatoid Arthritis Registry [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/association-of-rheumatoid-arthritis-related-autoantibodies-with-pulmonary-function-test-abnormalities-in-a-prospective-rheumatoid-arthritis-registry/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-of-rheumatoid-arthritis-related-autoantibodies-with-pulmonary-function-test-abnormalities-in-a-prospective-rheumatoid-arthritis-registry/