Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Behcet’s Disease (BD) is a systemic vasculitis characterized by involvement of vessels of any size and type. In the course systemic vasculitis, it is important to distinguish disease activity from damage to prevent unnecessary immunosuppression. Damage is also an important surrogate for long-term outcome in vasculitis. Although a well-established validated damage index, “vasculitis damage index” (VDI) is available for vasculitis, its performance in BD has never been assessed. In this study we assessed the damage in BD by using VDI, to determine whether VDI covers all BD-associated damage and lastly to develop a preliminary BD-specific damage index with the obtained data.
Methods: A total of 139 consecutive patients with BD (F/M: 58/81, mean age 38.9±10.9 yrs, disease duration 9.5±7.4 yrs) from a single center were evaluated for damage in a cross-sectional study using the VDI. Considering the patients data and items of VDI with further literature search for BD-specific damages, new items (detailed cardiovascular, ocular, and vascular involvement-, particularly venous disease-related damages) were added to VDI. This modified VDI (Behcet’s Disease-VDI [B-VDI]) was also scored in allpatients.
Results: Seventy seven patients (55.4%) had major organ involvement and 105 (75.5%) patients were on immunosupressive (IS) treatment (Table 1). The mean VDI score was 0.3±0.7 and majority of the patients had score “0” (“0” in 107 [77%], “1” in 22 [15.8%], “2” in 7 [5%], “3” in 1 [0.7%], and “4” in 2 [1.4%] patients). The mean B-VDI score was 0.6±1.1 (“0” in 92 [66.2%], “1” in 25 [18%], “2” in 13 [9.4%], “3” in 4 [2.9%] and “4” in 3 [2.2%] patients, “5” in 1 [0.7%], and “6” in 1 [0.7%] patient) and was significantly higher than VDI (p<0.001). The main difference between VDI and B-VDI was in vascular (0.05±0.2 vs 0.3±0.6, p<0.001) damage items. Both VDI and B-VDI scores were significantly higher in patients with major organ involvement compared to mucocutaneous BD. Both scores were also positively correlated with the age, disease duration and total duration of IS treatment. When individual organ items evaluated, it was observed that damage in patients with major organ involvement was predominantly associated with ocular and vascular involvements. Although VDI-eye and B-VDI-eye scores were not significantly different (both 0.3±0.6, p=0.32), B-VDI-vascular scores were significantly higher than VDI-vascular scores both in the entire cohort and in patients with major organ involvement (0.6±0.8 vs 0.1±0.3, p<0.001).
Conclusion: Both VDI and B-VDI capture reliable data on damage among patients with BD. However, VDI does not cover all vascular involvement-related damages of BD. Addition of new items, especially about vascular damage, to VDI will provide more comprehensive damage assessment in BD. Further prospective followup is required to determine the prognostic value of these damage indices in BD. 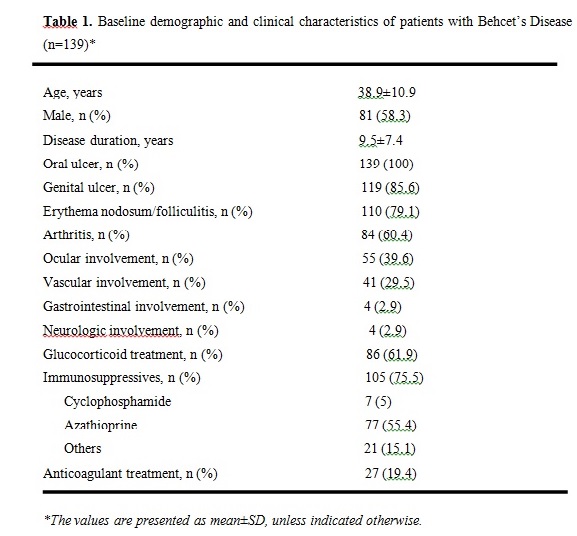
To cite this abstract in AMA style:
Unal AU, Yildirim HG, Cikikci C, Ozen G, Inanc N, Atagunduz P, Ergun T, Direskeneli H. Assessment of Damage in Behcet’s Disease: Do We Need a Specific Damage Index? [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/assessment-of-damage-in-behcets-disease-do-we-need-a-specific-damage-index/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessment-of-damage-in-behcets-disease-do-we-need-a-specific-damage-index/